A recent study from South Korea with 9.5 million participants (followed for 10 years) shows that changing to metabolic dysfunction–associated fatty liver disease (MAFLD) as a name change from nonalcoholic fatty liver disease (NAFLD) changes the prevalence of at-risk individuals.
Key findings:
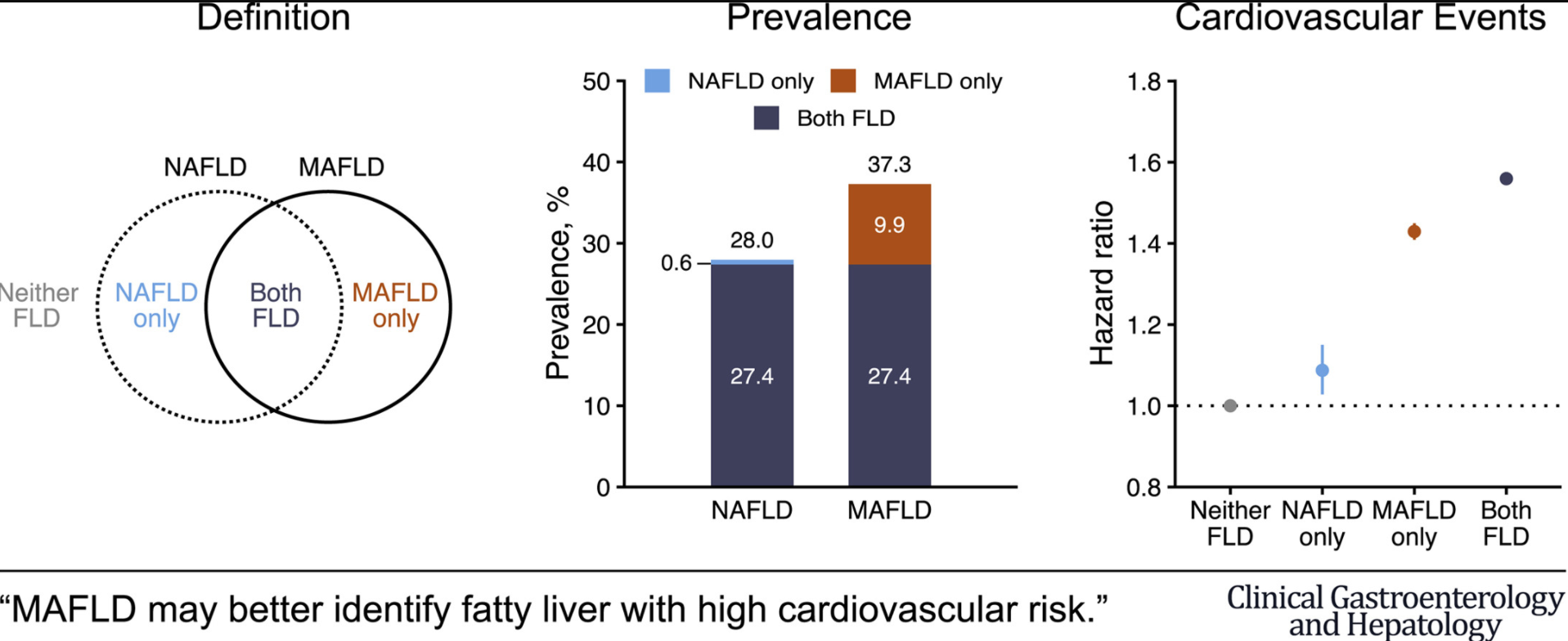
Prevalence of NAFLD and MAFLD were 28.0% and 37.3%, respectively
NAFLD and MAFLD were each associated with significantly higher risk for CVD events: multivariable-adjusted hazard ratios (95% confidence interval) for CVD events were 1.09 (1.03-1.15) in the NAFLD-only group, 1.43 (1.41-1.45) in the MAFLD-only group, and 1.56 (1.54-1.58) in the Both-FLD group
In the same issue, a study from Hong Kong showed similar prevalence rates between MAFLD (25.9%) and NAFLD (25.7%) (Clin Gastroenterol Hepatol 2021; 19: 2161-2171). This study noted that many people with hepatic steatosis at baseline have less severe metabolic burden.
Also, in the same issue, using a well-define population of more than 13,000 from NHANES III, this retrospective study (Clin Gastroenterol Hepatol 2021; 19: 2172-2181) found that Non-NAFLD MAFLD patients had the highest all-cause and cardiovascular-cause related mortality. In addition, this group had the highest rate of advanced fibrosis >7% (compared to <2% in other groups.
My take (borrowed from authors of first study): “The change from NAFLD to MAFLD criteria may identify a greater number of individuals with metabolically complicated fatty liver and increased risk for CVD.”
MAFLD is diagnosed based on the presence of hepatic steatosis with one or more of the following:
diabetes mellitus
overweight/obesity (BMI >/= 23)
at least 2 metabolic abnormalities: a) Waist circumference ≥90 cm in men and 80 cm in women. b) Blood pressure ≥130/85 mmHg or under anti-hypertension therapy. c) High-density lipoprotein cholesterol (HDL-C) <40 mg/dL for males and <50 mg/dL for females. d) Triglyceride (TG) ≥150 mg/dL or specific drug treatment. e) fasting glucose ≥100 f) Homeostasis model assessment-insulin resistance (HOMA-IR) score ≥2.5; and g) Hypersensitive C-reactive protein (hs-CRP) level >2 mg/L.
NAFLD Criteria in this study:
The presence of hepatic steatosis without 1. excessive drinking ( ≥30 g/day in men, ≥20 g/day in women) and 2. concomitant liver diseases