- J Hou et al. NEJM 2026. DOI: 10.1056/NEJMoa251513. Phase 3 Results of Bepirovirsen Treatment for Chronic Hepatitis B Virus Infection
- A Lok. NEJM 2026. DOI: 10.1056/NEJMe2605575. A Major Step toward a Cure for Hepatitis B Infection (editorial)
Methods:
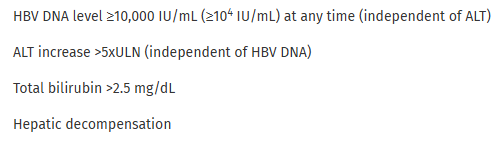
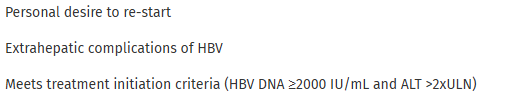
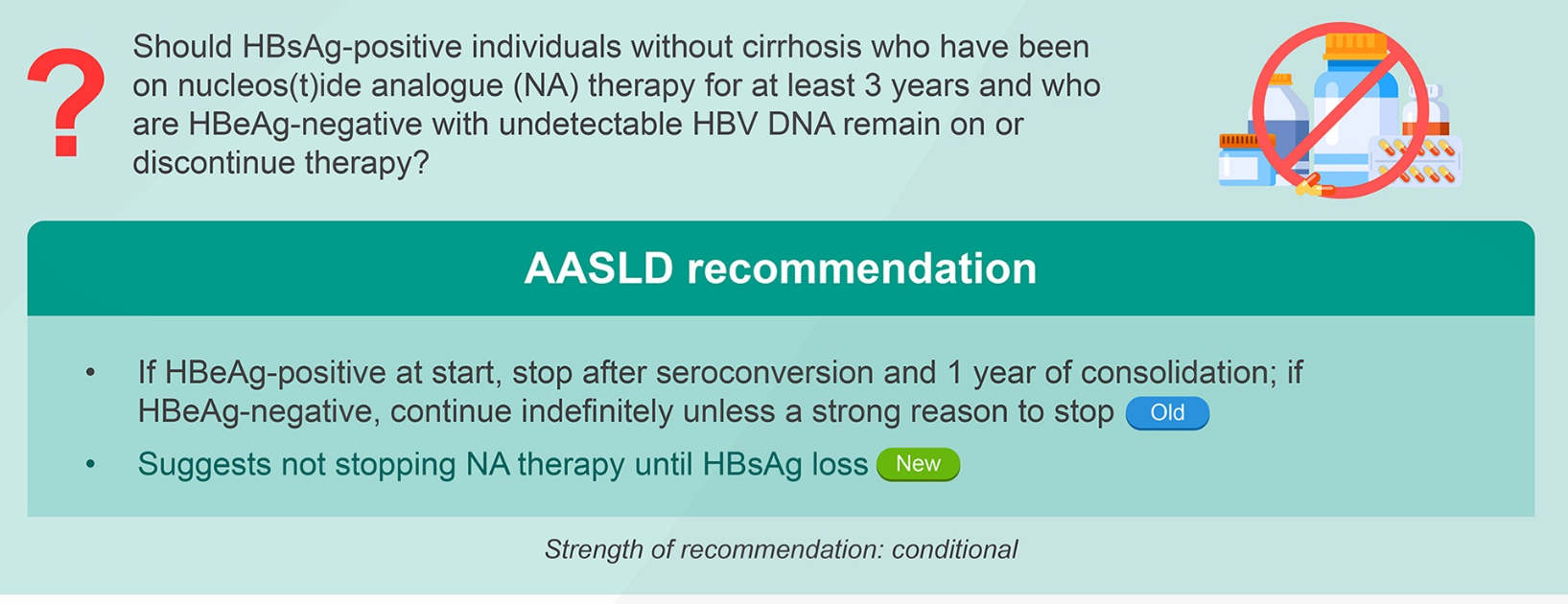
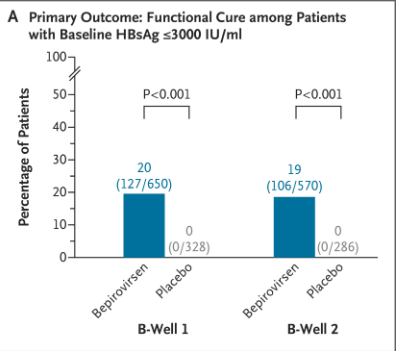
The B-Well trials enrolled patients with noncirrhotic chronic hepatitis B with suppressed HBV DNA during receipt of NA therapy and a low HBsAg level (≤3000 IU per milliliter). A total of 1838 patients were randomly assigned in a 2:1 ratio to receive bepirovirsen or placebo administered as a weekly subcutaneous injection for 24 weeks. The patients who had undetectable HBsAg and unquantifiable HBV DNA from week 24 to week 46 were eligible to discontinue NA therapy at week 48. The primary outcome of a functional cure was assessed at week 72.
Key findings:
- In two phase 3 trials, 19% of patients with chronic hepatitis B infection had a functional cure with the antisense oligonucleotide bepirovirsen, 24 weeks after stopping all HBV treatment; functional cure was not seen with placebo.
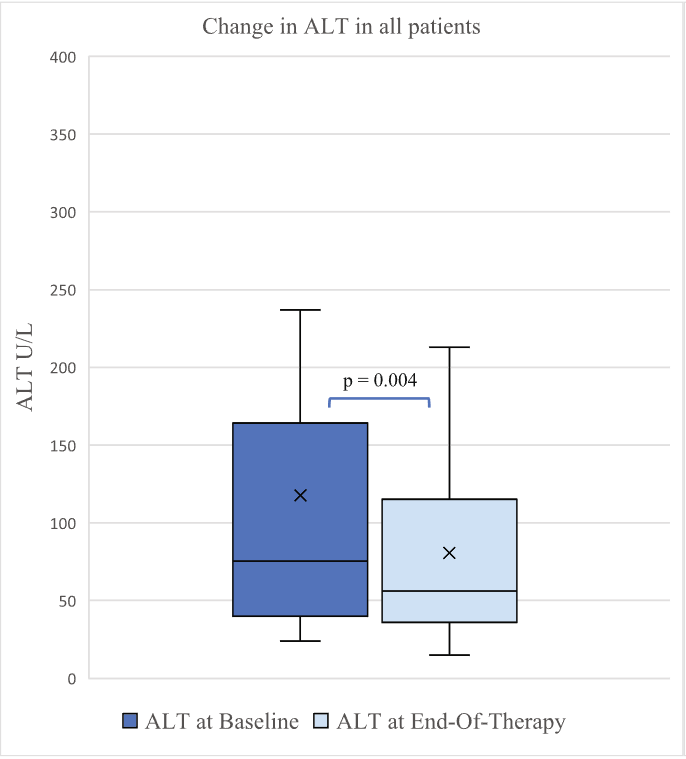
Adverse events of grade 3 or higher were more common in the bepirovirsen groups than in the placebo groups (16% vs. 3%), with an increase in alanine aminotransferase (ALT) being the most common (6%) with bepirovirsen. In addition, adverse events requiring a dose interruption or delay were reported in 16% of the patients in the bepirovirsen groups as compared with 2% in the placebo groups.
My take:
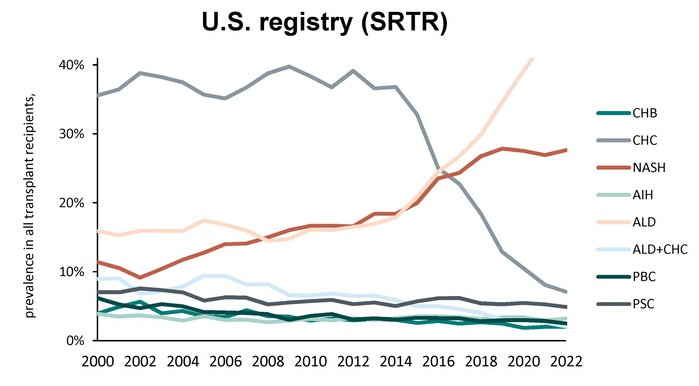
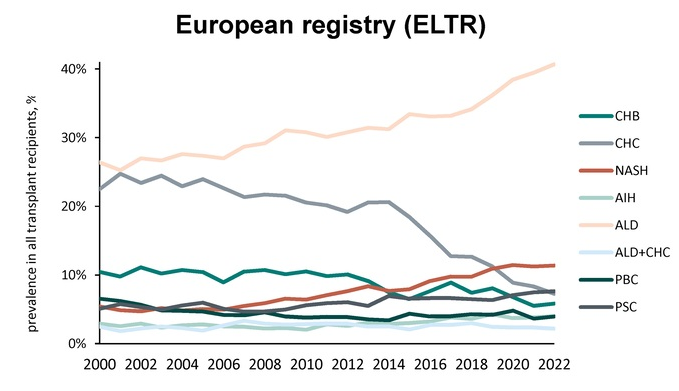
- Currently, it is estimated that 240 million persons worldwide are living with chronic HBV. These trials represent a big step forward showing that many patients can achieve a functional cure (no detectable HBV) off all medications. Prevention of HBV, though, via immunization holds much more promise in reducing the number of individuals with poor outcomes due to HBV.
- Several of the adverse events — an increase in the levels of ALT and creatinine and a decrease in the platelet count — can be potentially serious if stringent monitoring (every 1 to 2 weeks) and strict trial-adopted guidelines regarding the pausing of therapy are not followed.
Related blog posts:
- New Age for Hepatitis B Therapies (2022 Bepirovirsen Phase 2b study)
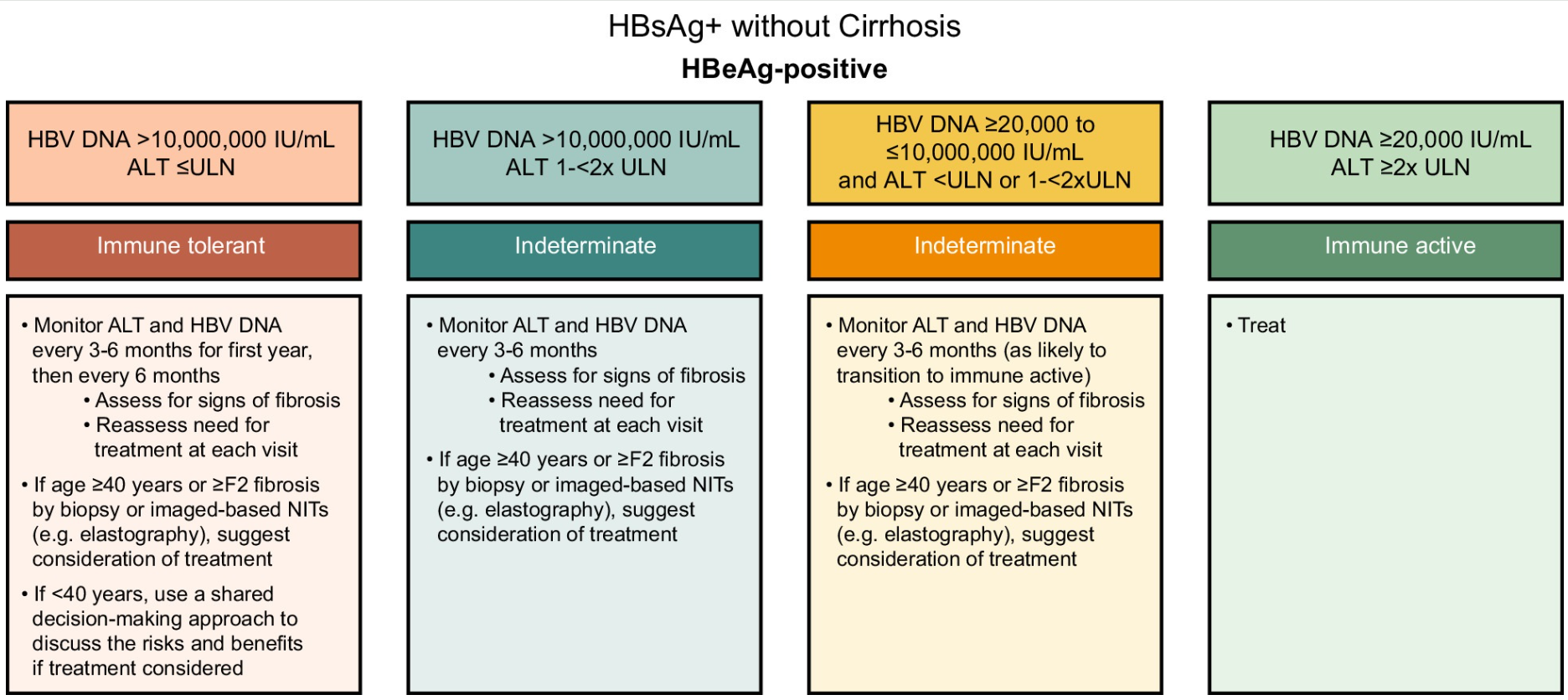
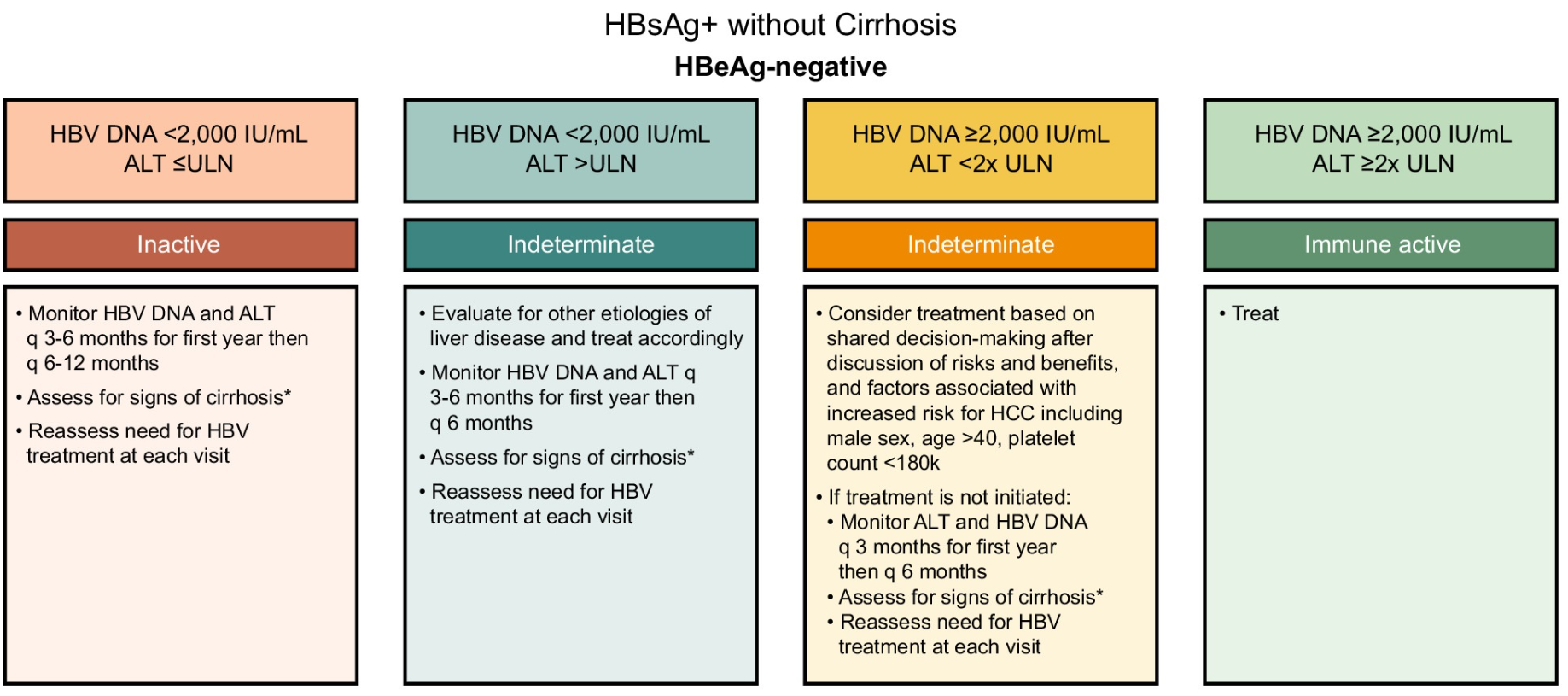
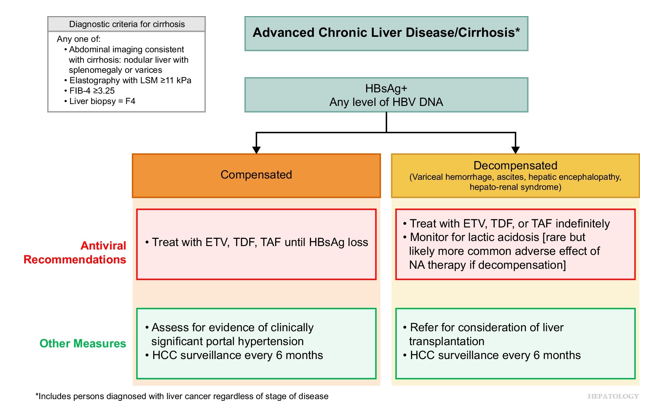
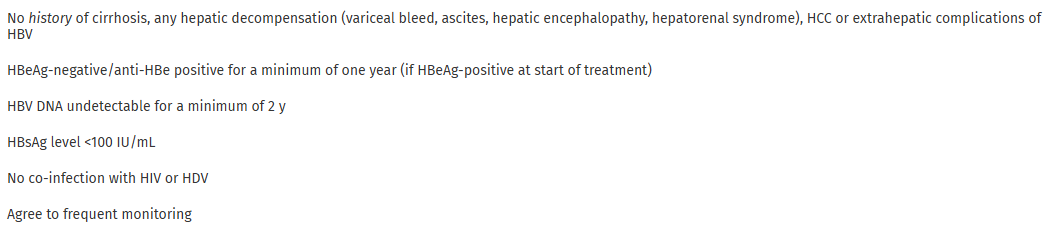
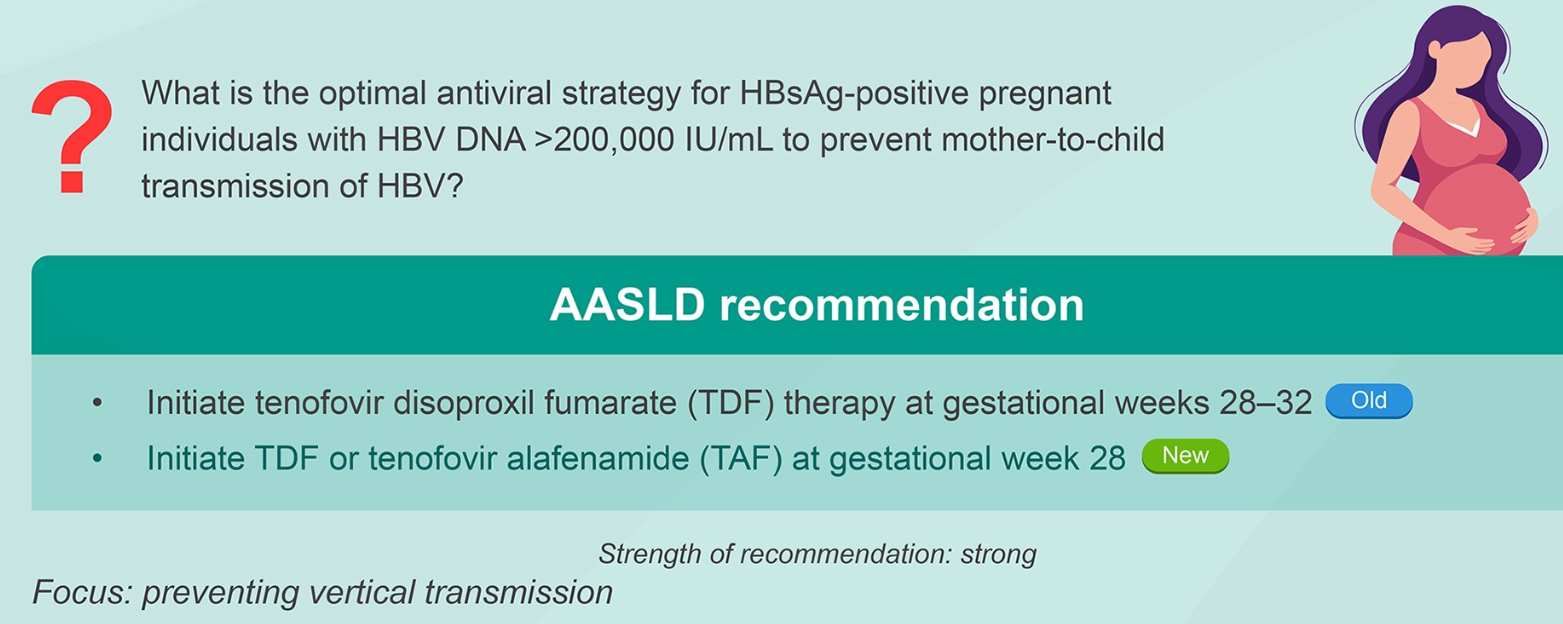
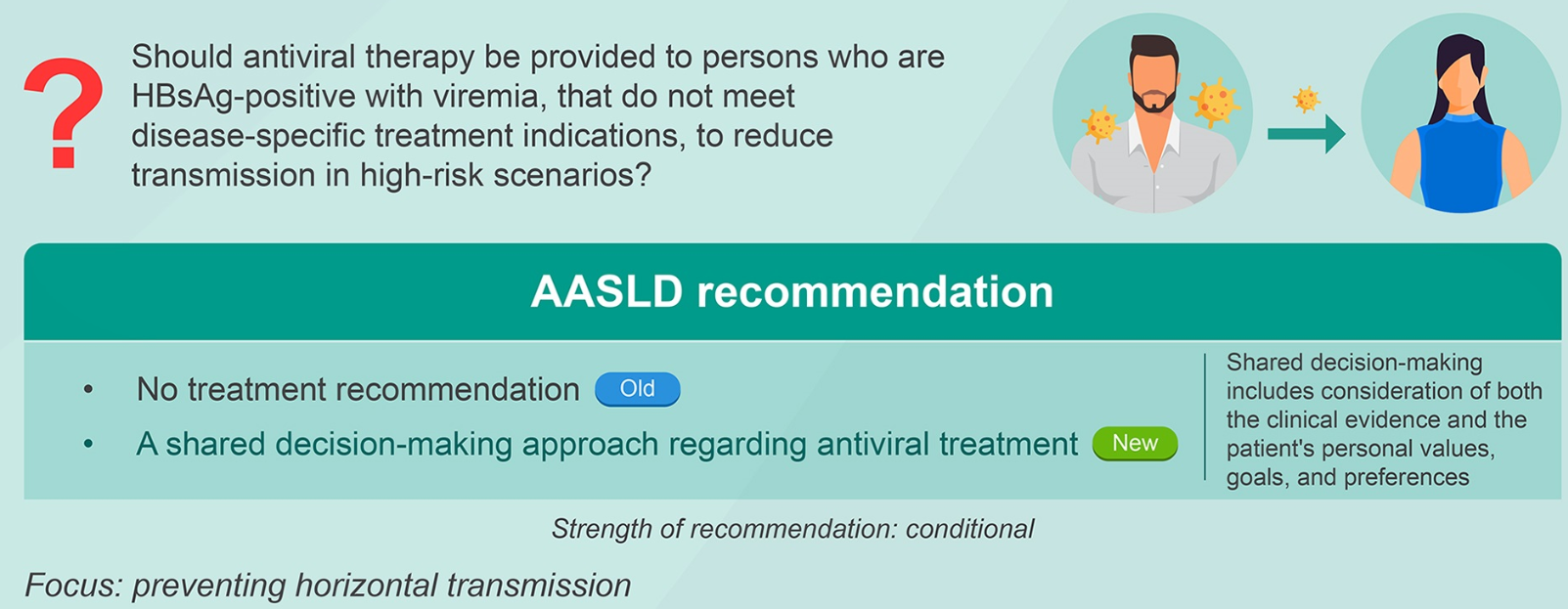
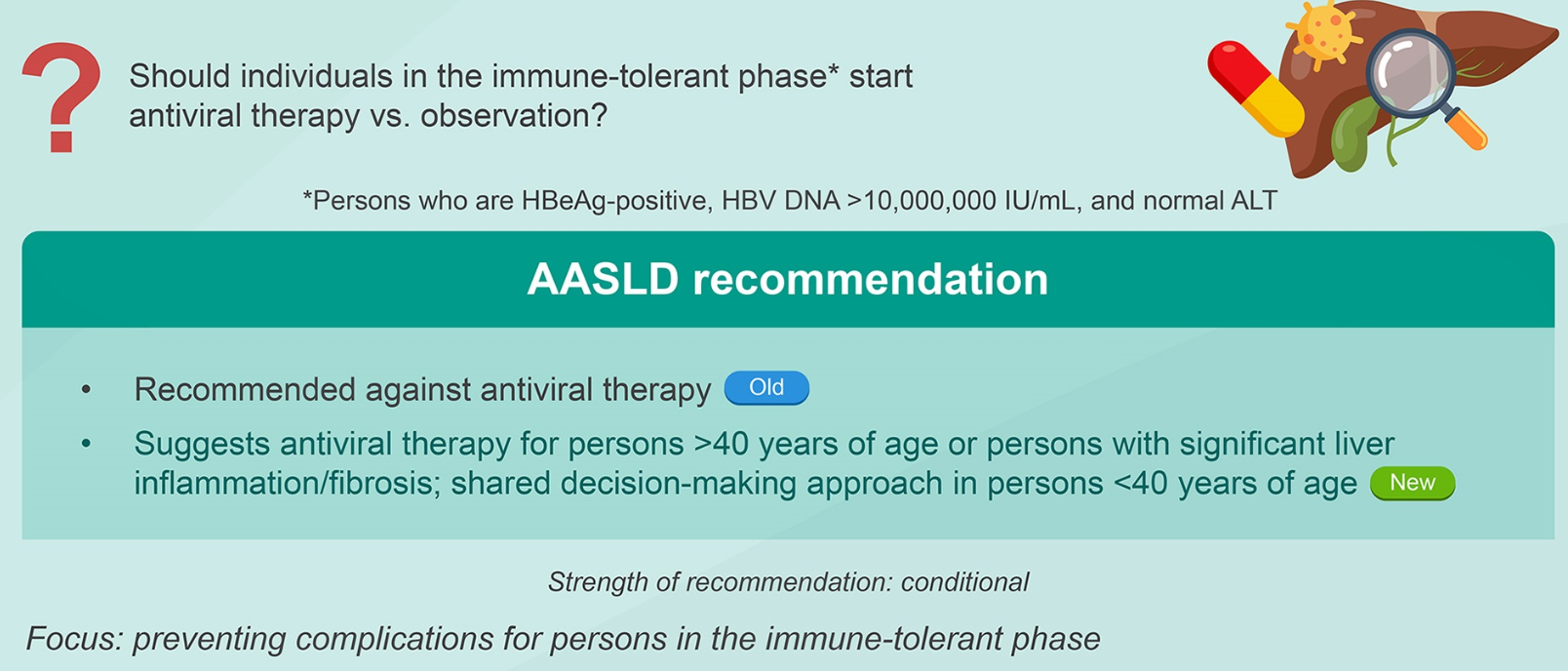
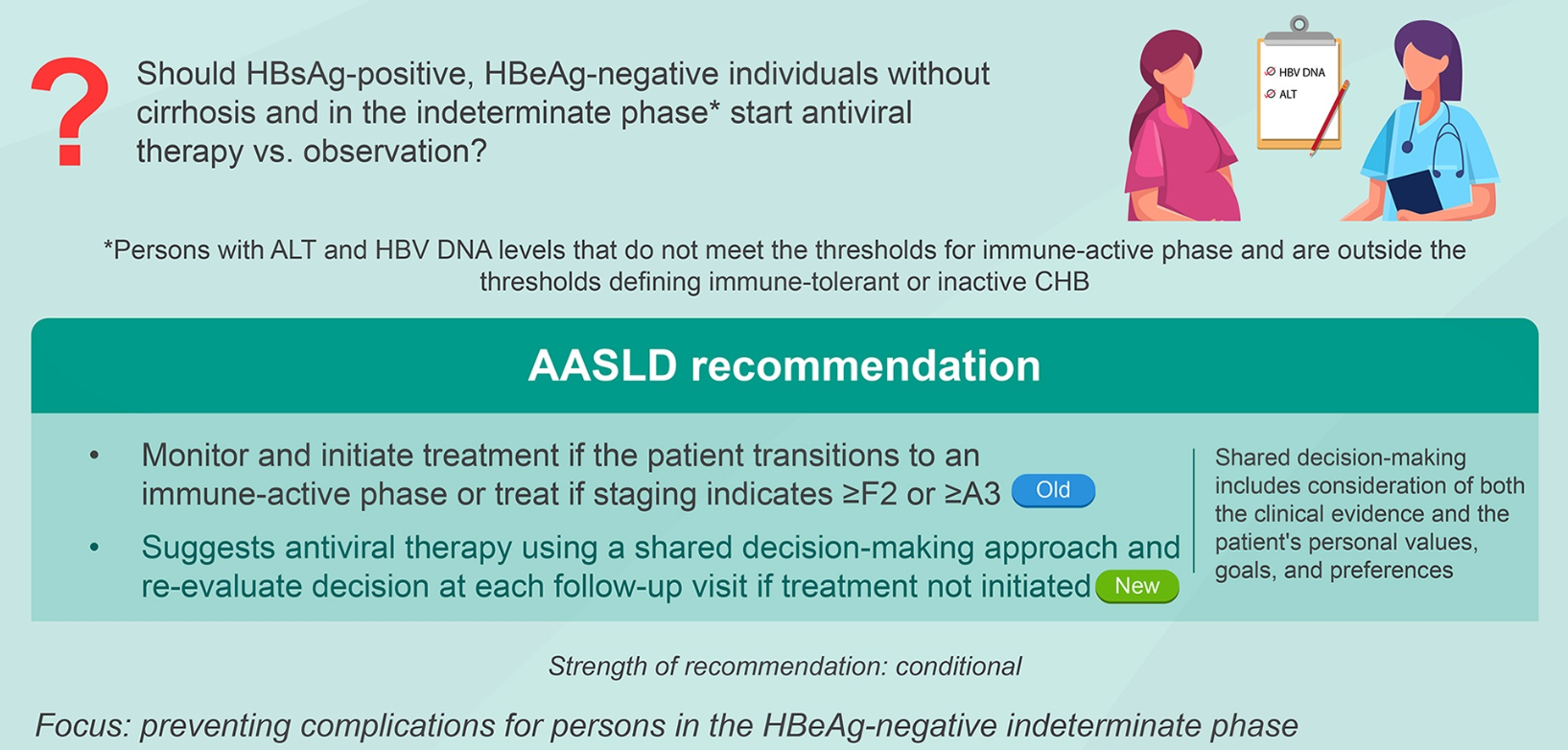
- Major Update on AASLD IDSA Practice Guideline on Treatment of Chronic Hepatitis B (Part 1)
- Major Update of AASLD IDSA Practice Guideline on Treatment of Chronic Hepatitis B (Part 2)
- Scientific Basis for Current Hepatitis B Vaccine Strategy