A Kaplan et al. Liver Transplantation 2025; 31: 1165-1175. Open Access! The rising cost of liver transplantation in the United States
Key points:
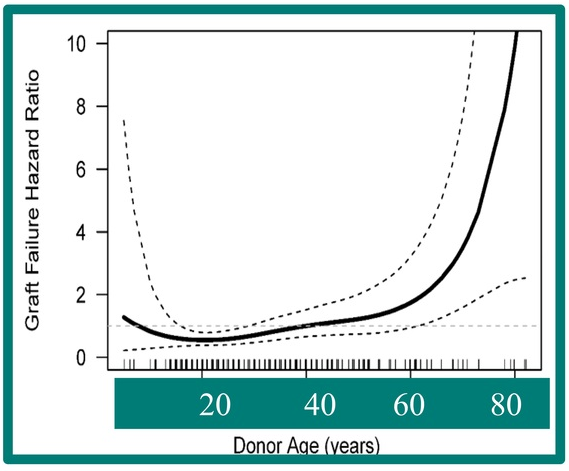
- LT is resource-intensive and costly, with expenditures rising dramatically in recent years. Factors contributing to this increase in cost include expanded transplant criteria (higher risk recipients), utilization of marginal organs, and broader organ distribution, resulting in significant logistical expenses
- Advanced technologies like organ perfusion devices, while promising better outcomes, further inflate costs due to their high price and market monopolization
- Despite rising costs, reimbursement has remained largely stagnant, putting financial strain on transplant programs, and threatening their sustainability. “In fact, there has been an observed decline (−32%) in adjusted reimbursement of LT by Medicare over the past decade.62“
Increased Costs Associated with Recipient Characteristics:
- “According to the latest annual SRTR report, patients aged 65 or older undergoing LT accounted for 21.9% of transplants in 2022, up from 14.6% a decade prior.18 One study looking at the cost burden of hospitalizations associated with liver transplants from 2016 to 2019 found mean costs increasing by nearly $10,000 per hospitalization in the group aged >65 over the study period”
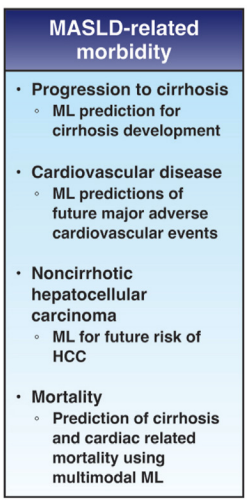
- “Increasing numbers of patients are being transplanted for steatotic liver disease… LT associated with metabolic dysfunction–associated steatotic liver disease has been demonstrated to be associated with higher costs, largely attributable to longer posttransplant lengths of stay.21–23 Similarly, LT associated with AH/ALD is very expensive—at 1 transplant program, net revenue from LT admission to 90 days after LT was −5.0% for AH compared to +1.4% for acute-on-chronic liver failure.24“
Organ distribution:
- “In 2019, the OPTN implemented further changes in liver allocation from a regional-based system to an acuity circle model. This model was intended to create a more equitable allocation system and to reduce waitlist mortality for patients across the United States…This has been associated with a 77% increase in fly-out costs, amounting to an increase in $47,010,190 across all LT centers by recent estimates.4“
- “1 study found that the cost for private jets ranged from $6850 to $27,350 depending on the distance traveled.29 In this same study, commercial flights, as opposed to private jets, were found to be safe and only around 10% of the cost.”
Perfusion devices:
“The FDA’s approval of organ perfusion and preservation devices has ushered in a new era in organ transplantation, enabling medical teams to extend the geographical reach for organ procurement. These devices enhance the utilization of organs that may have previously been discarded… It has been suggested that the average cost of using normothermic regional perfusion for DCD organs is around $10,000 per donor, compared to the $40,000–$80,000 per donor for use of NMP [normothermic machine perfusion].”
My take: Transplant centers are getting squeezed financially. In addition, ~25% of liver transplant patients experience a high financial burden. Pretty soon, along with checking organs for suitability, it may be necessary to assess liver transplant centers for viability.
Related blog posts:
- Costs and Opportunity Costs in Pediatric Liver Transplantation
- Liver Shorts: Relationship of Hepatic Steatosis to Cardiovascular Disease and the Cost of Liver Transplantation
- Fairness Lost: The Shift in Organ Transplant Practices
- Financial Toxicity of Liver Transplantation and Cirrhosis