A total of 46 studies fulfilled the eligibility criteria, comprising approximately 8 million participants from 21 countries.
Key findings:
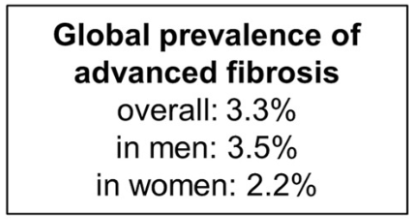
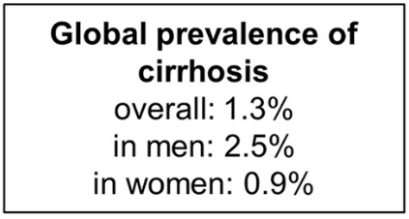
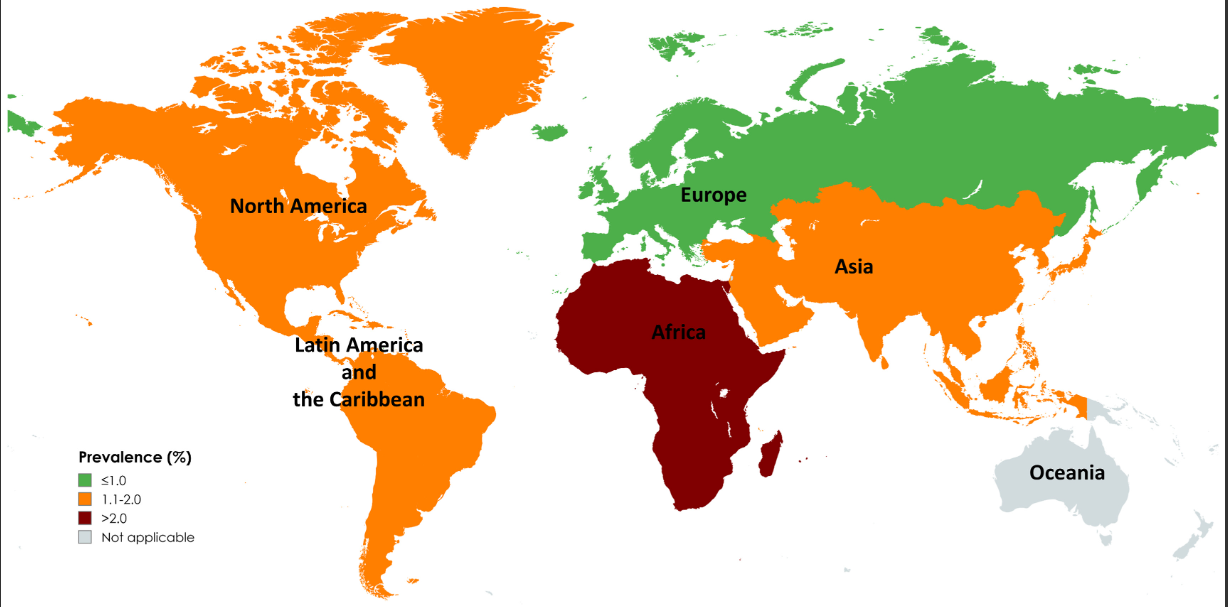
The pooled prevalence rates of advanced liver fibrosis and cirrhosis in the general population were 3.3% (95% CI, 2.4%–4.2%) and 1.3% (95% CI, 0.9%–1.7%) worldwide, respectively
Risk factors for cirrhosis were viral hepatitis, diabetes, excessive alcohol intake, obesity, and male sex
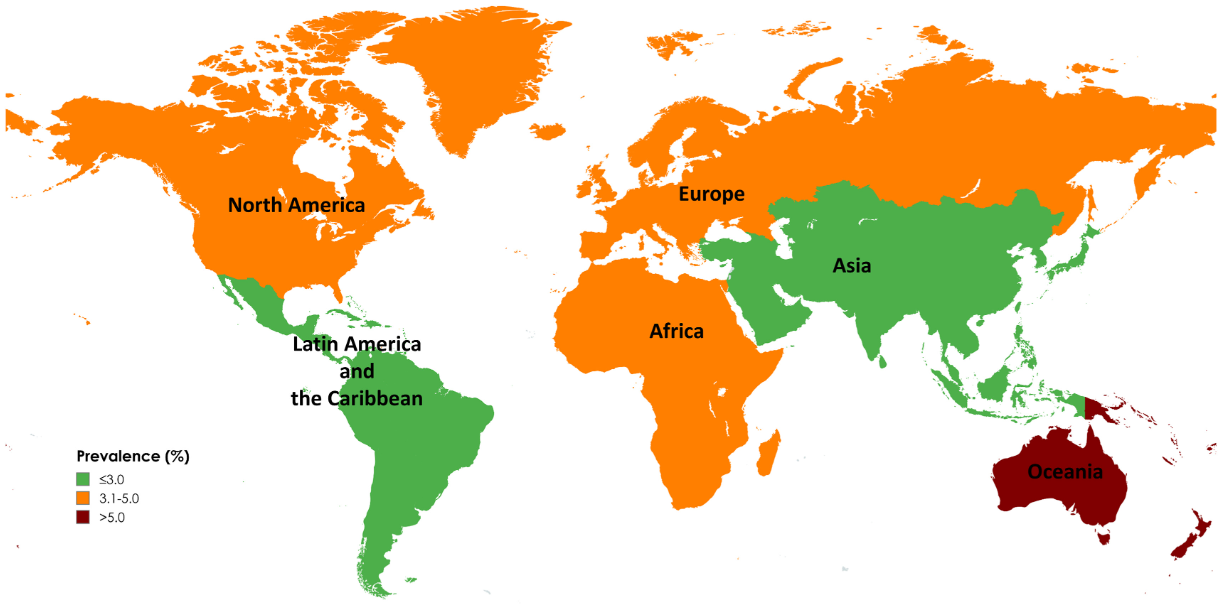
Limitations: 1. All included studies used noninvasive tests to diagnose advanced fibrosis and cirrhosis, which might overestimate prevalence in general populations. The diagnostic performance of these tests is influenced by baseline prevalence, leading to a higher rate of false positives in low-prevalence populations 2. Significant differences in prevalence by geographic region and time period. However, these differences could be influenced by variations in health care infrastructure, access to health care, and disease awareness, which may only partially reflect the true prevalence of advanced liver fibrosis and cirrhosis. In addition, the data is influenced by the number of studies (eg. Oceania had only 1 individual study).
Map of Global Prevalence of Advanced FibrossiMap of Global Prevalence of Cirrhosis
My take: This study provides estimates of the high and increasing prevalence of advanced liver fibrosis and cirrhosis. This data is essential in determining if we are making progress and how to mitigate the disorders leading to advanced liver disease.
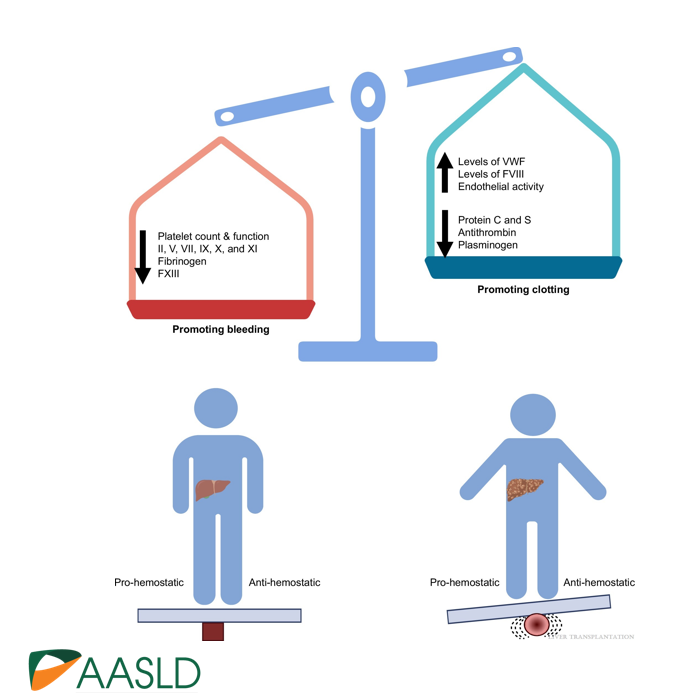
Background: “The most important factor contributing to bleeding risk in patients with liver disease is related to the presence of portal hypertension rather than coagulation abnormalities.1 The changes in the coagulation system in patients with cirrhosis create a re-balanced state, which is prothrombotic. Despite this well-known pathophysiology and recommendation against routine transfusion of blood products (especially fresh frozen plasma) by major guidelines, platelet and fresh frozen plasma transfusion remain a common practice before percutaneous liver procedures.2,3“
Methods: In this retrospective study from three centers in Spain, the researchers enrolled 1797 adults including 316 with cirrhosis (97% had compensated disease). They established a protocol that allowed, at the discretion of the radiologist, to transfuse patients with FFP or platelets if INR was 1.5 or greater or if platelets were 50,000 or below. The primary outcome of the study was major bleeding, which was defined as a drop in hemoglobin (2 or more units) or a need for transfusion of 2 or more units of blood within 1 week after the procedure. This study enrolled patients who underwent percutaneous liver biopsy (86% of cohort) and percutaneous ablation of liver tumors (14% of cohort). Only 6/25 (24%) with INR >1.5 received FFP. 16/22 (72%) with platelet counts below 50,000 received a platelet transfusion. Overall, 7 patients received FFP (1 with cirrhosis, 6 without) and 35 patients received platelets (16 with cirrhosis, 19 without).
Key findings:
Only 14 patients (0.8%) experienced major bleeding after the procedure, and there was no difference between those who had a diagnosis of cirrhosis versus those without cirrhosis. Bleeding occurred in 0.6% of patients with cirrhosis compared to 0.8% of those without.
Only 1 patient with an ablation procedure had major bleeding
Patients with a diagnosis of cirrhosis were more likely to receive a transfusion of any kind
Among those with major bleeding, none met the criteria for transfusion. That is, “no variable was identified to predict the risk of major bleeding.”
My take (borrowed from editorial): This study reinforces the recommendation that “correction of coagulation markers before procedures is unnecessary.”
The editorial notes that “the changes in the coagulation system in patients with cirrhosis create a re-balanced state, which is prothrombotic.
Related blog posts:
Time to Adjust the Knowledge Doubling Curve in Hepatology This post summarizes the following reference: PG Northup et al. Hepatology 2021; 73: 366-413 (346 references) Full text: Vascular Liver Disorders, Portal Vein Thrombosis, and Procedural Bleeding in Patients With Liver Disease: 2020 Practice Guidance by the American Association for the Study of Liver Diseases PDF version: Vascular Liver Disorders, Portal Vein Thrombosis, and Procedural Bleeding in Patients With Liver Disease: 2020 Practice Guidance by the American Association for the Study of Liver Diseases. Specific recommendations from this practice guidance: –For Platelets in the setting of cirrhosis: “Given the low risk of bleeding of many common procedures, potential risks of platelet transfusion, lack of evidence that elevating the platelet count reduces bleeding risk, and ability to use effective interventions, including transfusion and hemostasis if bleeding occurs, it is reasonable to perform both low‐ and high‐risk procedures without prophylactically correcting the platelet count...An individualized approach to patients with severe thrombocytopenia before procedures is recommended because of the lack of definitive evidence for safety and efficacy of interventions intended to increase platelet counts in patients with cirrhosis.” The authors note in Table 4, that the AASLD does not have a specific threshold for platelets, whereas other societies have used values of >30 or >50. –For INR in setting of cirrhosis: “The INR should not be used to gauge procedural bleeding risk in patients with cirrhosis who are not taking vitamin K antagonists (VKAs)…Measures aimed at reducing the INR are not recommended before procedures in patients with cirrhosis who are not taking VKAs…FFP transfusion before procedures is associated with risks and no proven benefits.”
In his book, Critical path, Buckminster Fuller (Fuller 1981), American architect, systems theorist, author, designer, inventor, and futurist, created the ‘knowledge doubling curve’. He noticed that until 1900 human knowledge doubled approximately every century and by the end of World War II knowledge was doubling every 25 years (Knowledge is not everything, Paul Chamberlain). Now the doubling of knowledge, in the age of the internet and social media, has become even shorter, perhaps less than a year.
I was thinking about this knowledge doubling curve after reading two practice guidances in a recent issue of Hepatology:
The first guidance is mainly for reference as pediatric gastroenterologists do not focus on reproductive health. The authors do provide guidance on contraceptive options which is an important topic for adolescents. The main guidance is disease-specific information for pregnancy in the setting of underlying liver conditions including liver transplantation, cirrhosis, viral hepatitis, autoimmune hepatitis, PSC, PBC, Wilson’s disease, hepatitis C, nonalcoholic fatty liver disease, HELLP, acute fatty liver disease of pregnancy, Budd-Chiari, FNH, hepatocellular adenoma, and others. The guidance also provides recommendations for how to evaluate abnormal liver tests in pregnancy and reviews liver medications during pregnancy (Table 4).
The second guidance reviews the following:
An overview of the current understanding of bleeding and thrombosis in cirrhosis.
An evidence‐based justification for bleeding risk assessment in patients with cirrhosis before invasive procedures, including current concepts in preprocedural testing and laboratory analysis and their role in predicting bleeding complications.
An outline of established and recently identified risk factors for venous thrombosis in the portal and hepatic venous systems in both patients with and without cirrhosis along with thrombophilia testing recommendations.
A review of the strengths and weaknesses of the various classification systems for portal vein thrombosis and a proposal for standard nomenclature regarding characterization of portal vein thrombosis location, time course, and progression.
Useful points:
In patients with cirrhosis, there are “complex hemostatic changes that are not adequately captured by traditional laboratory measures of hemostasis, such as PT, aPTT, and platelet count.”
“Because of conflicting data in the literature, there is no data-driven specific INR or platelet cut-off in which procedural bleeding risk is reliable increased.” In some studies, the authors conclude that “that the low platelet count may have been merely a reflection of advanced portal hypertension and not a causative risk factor for bleeding.”
For Platelets in the setting of cirrhosis: “Given the low risk of bleeding of many common procedures, potential risks of platelet transfusion, lack of evidence that elevating the platelet count reduces bleeding risk, and ability to use effective interventions, including transfusion and hemostasis if bleeding occurs, it is reasonable to perform both low‐ and high‐risk procedures without prophylactically correcting the platelet count...An individualized approach to patients with severe thrombocytopenia before procedures is recommended because of the lack of definitive evidence for safety and efficacy of interventions intended to increase platelet counts in patients with cirrhosis.” The authors note in Table 4, that the AASLD does not have a specific threshold for platelets, whereas other societies have used values of >30 or >50.
For INR in setting of cirrhosis: “The INR should not be used to gauge procedural bleeding risk in patients with cirrhosis who are not taking vitamin K antagonists (VKAs)…Measures aimed at reducing the INR are not recommended before procedures in patients with cirrhosis who are not taking VKAs…FFP transfusion before procedures is associated with risks and no proven benefits.”
The guidance lists a step‐by‐step treatment and surveillance algorithm for portal vein thrombosis in patients with cirrhosis (and without cirrhosis).
The guidance provides updated diagnostic, treatment, and management recommendations for sinusoidal obstruction syndrome (formerly known as hepatic-veno-occlusive disease), hereditary hemorrhagic telangiectasia, and hepatic vein thrombosis (aka Budd-Chiari).
Classification and management recommendations for idiopathic noncirrhotic portal hypertension and the portosinusoidal vascular disorders.
Surveillance and evaluation recommendations for hepatic and splenic artery aneurysms.
A review of the management issues in vascular liver disorders specific to children and guidance on early intervention in extrahepatic portal vein obstruction in children.
My take: In essence, these two articles are condensed textbooks. The first on Liver Disease, Pregnancy and Reproductive Health. And the second on Bleeding in the Setting of Chronic Liver Disease and Vascular Liver Diseases.
Below I’ve included some of my notes and slides. There may be errors of omission or transcription.
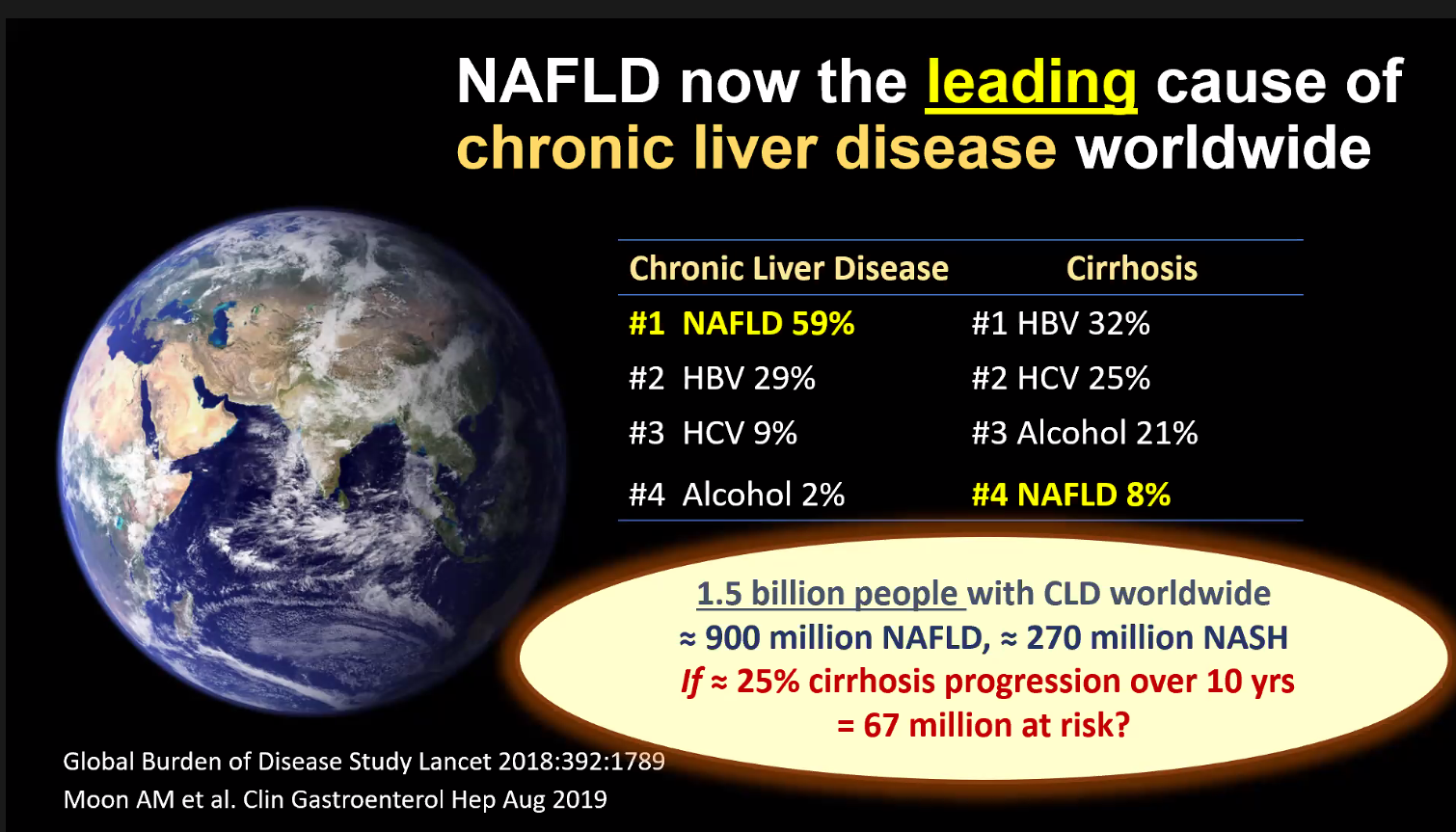
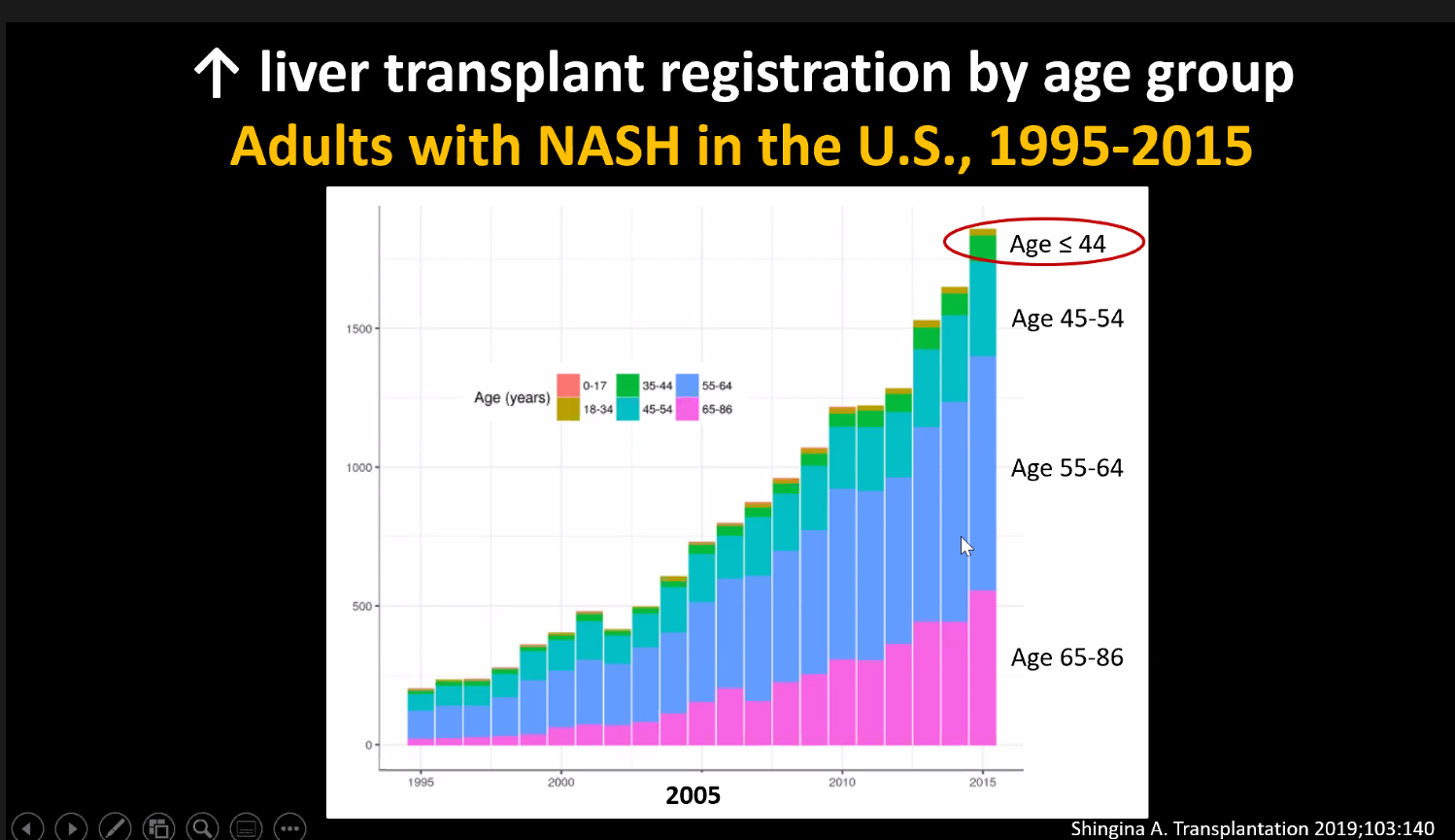
What’s Hot? NAFLD and NASH Stavra Xanthakos
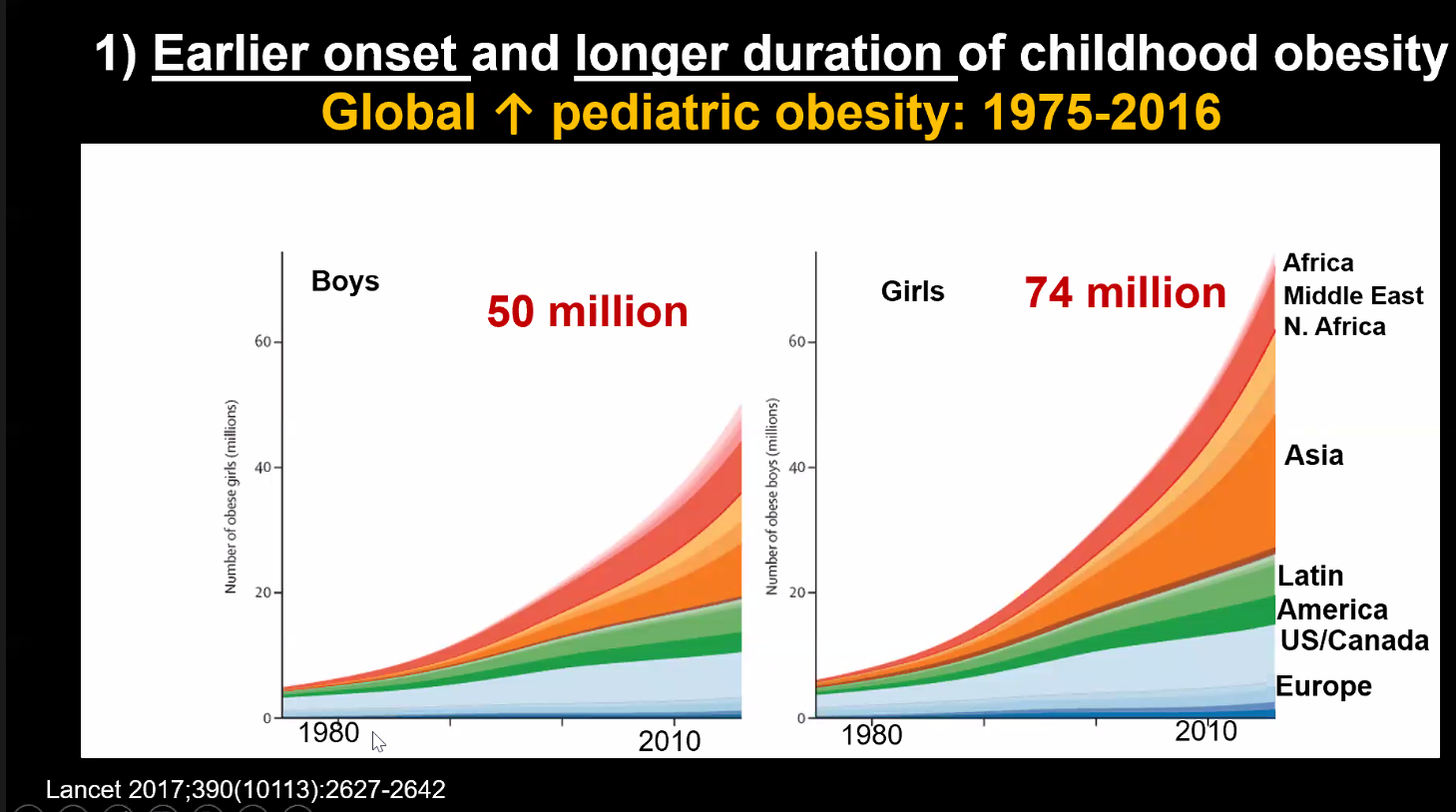
Fatty liver disease burden of NAFLD and NASH is increasing. This increases the rate of cirrhosis, liver cancer and liver transplantation; the latter is being needed at younger ages
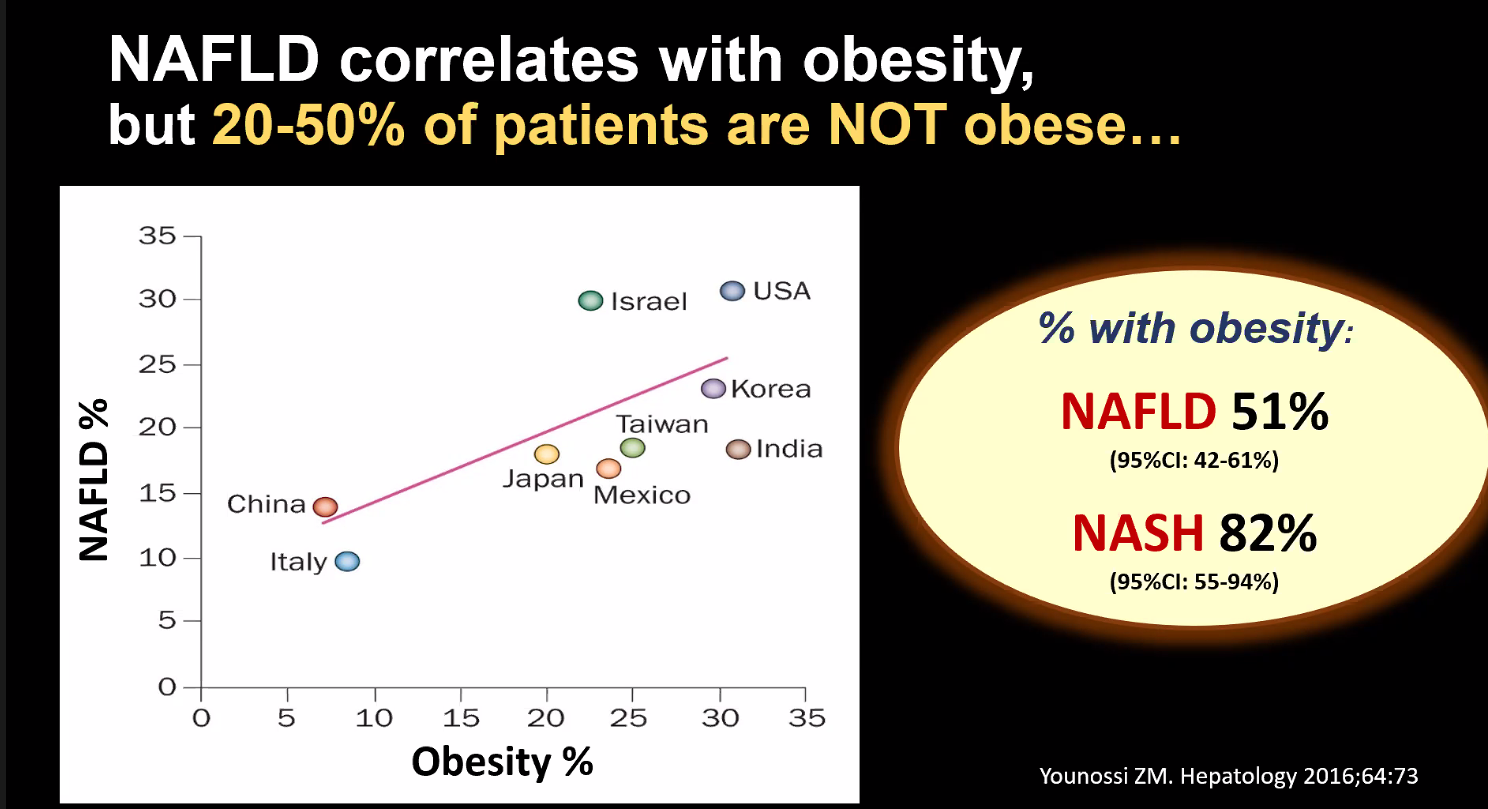
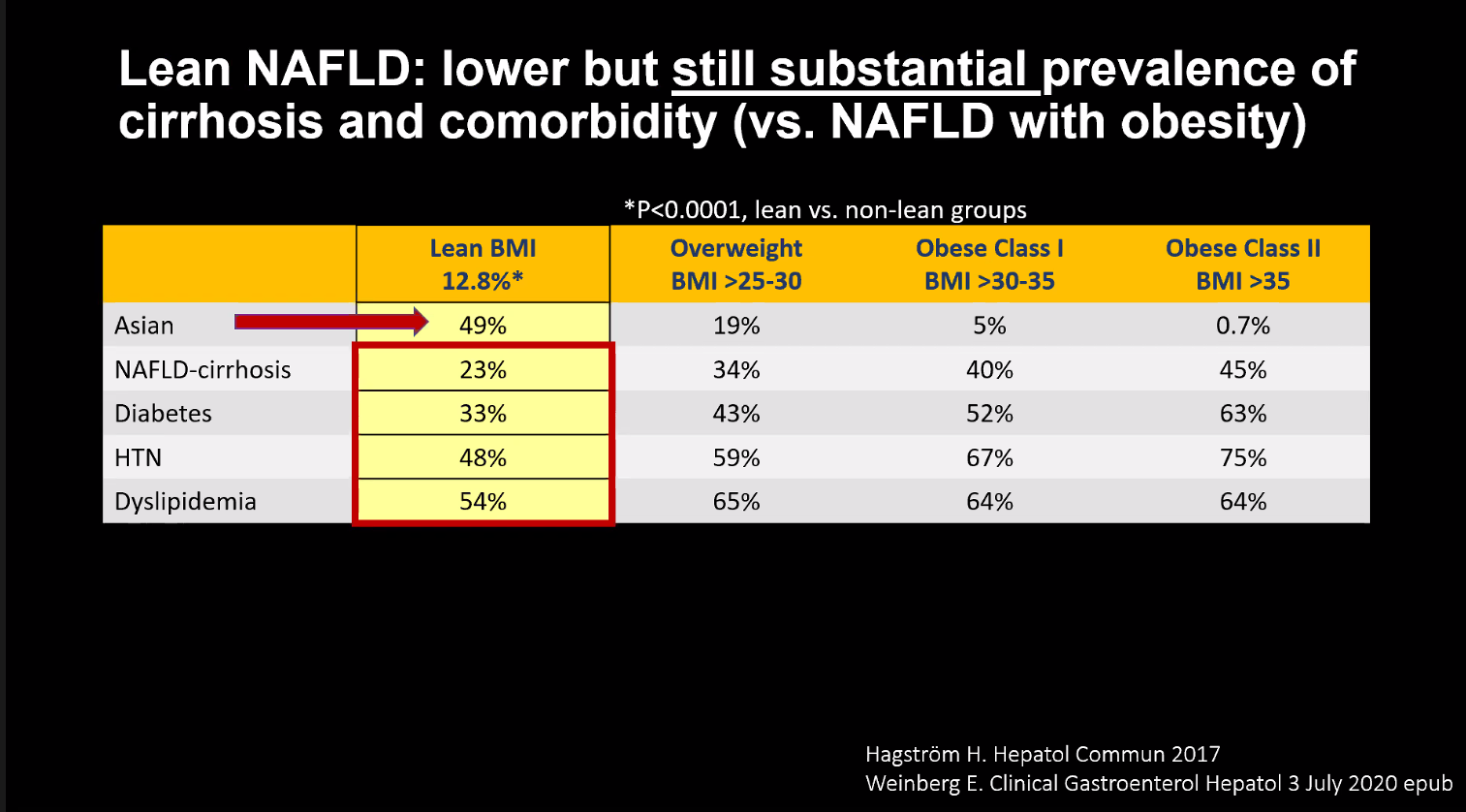
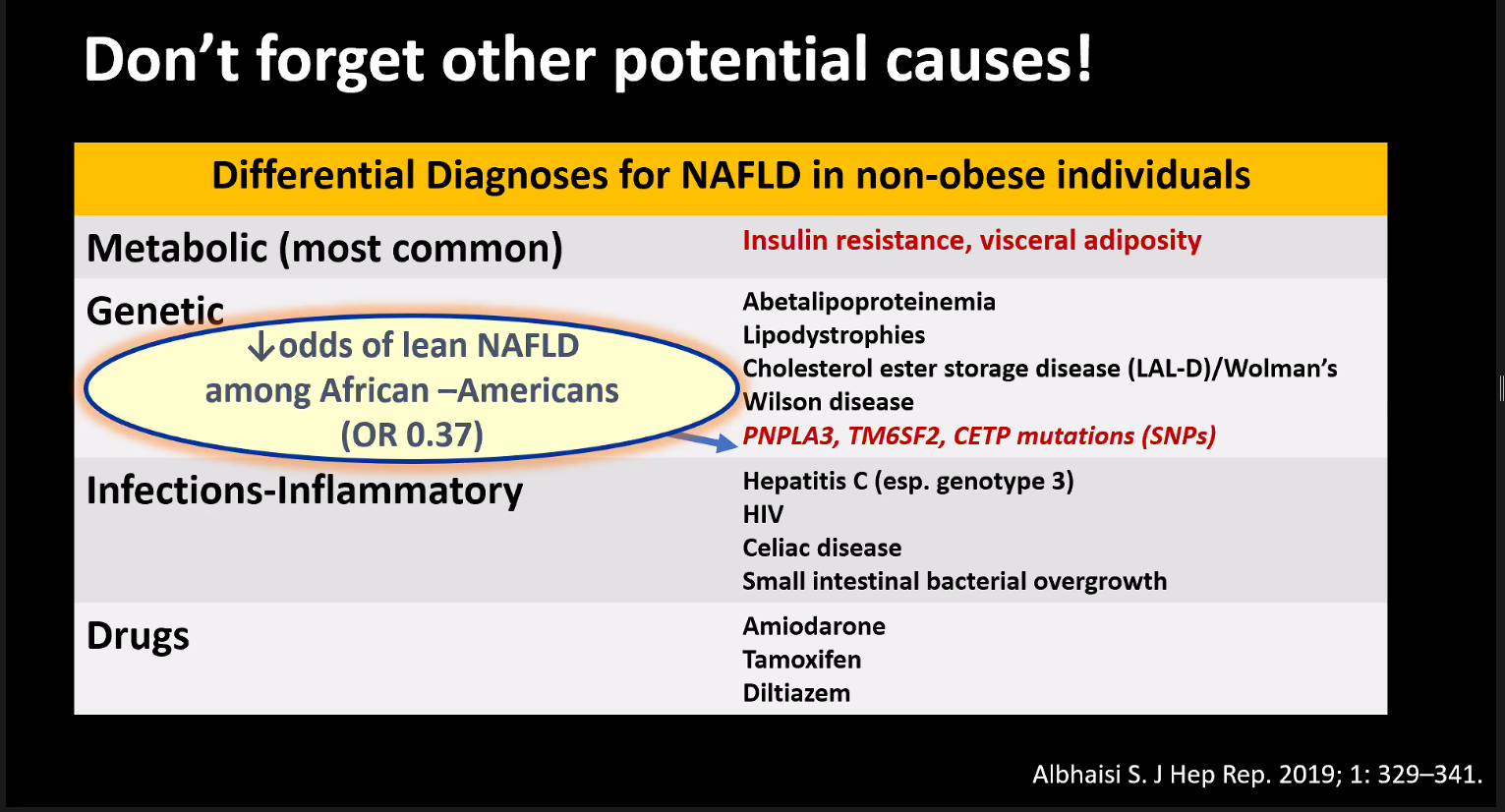
Explained that “Lean” (normal BMI) NAFLD is common
Diabetes is strongest risk factor for severe fatty liver disease (NASH or fibrosis). PNPLA3 is genetic risk factor for NAFLD risk.
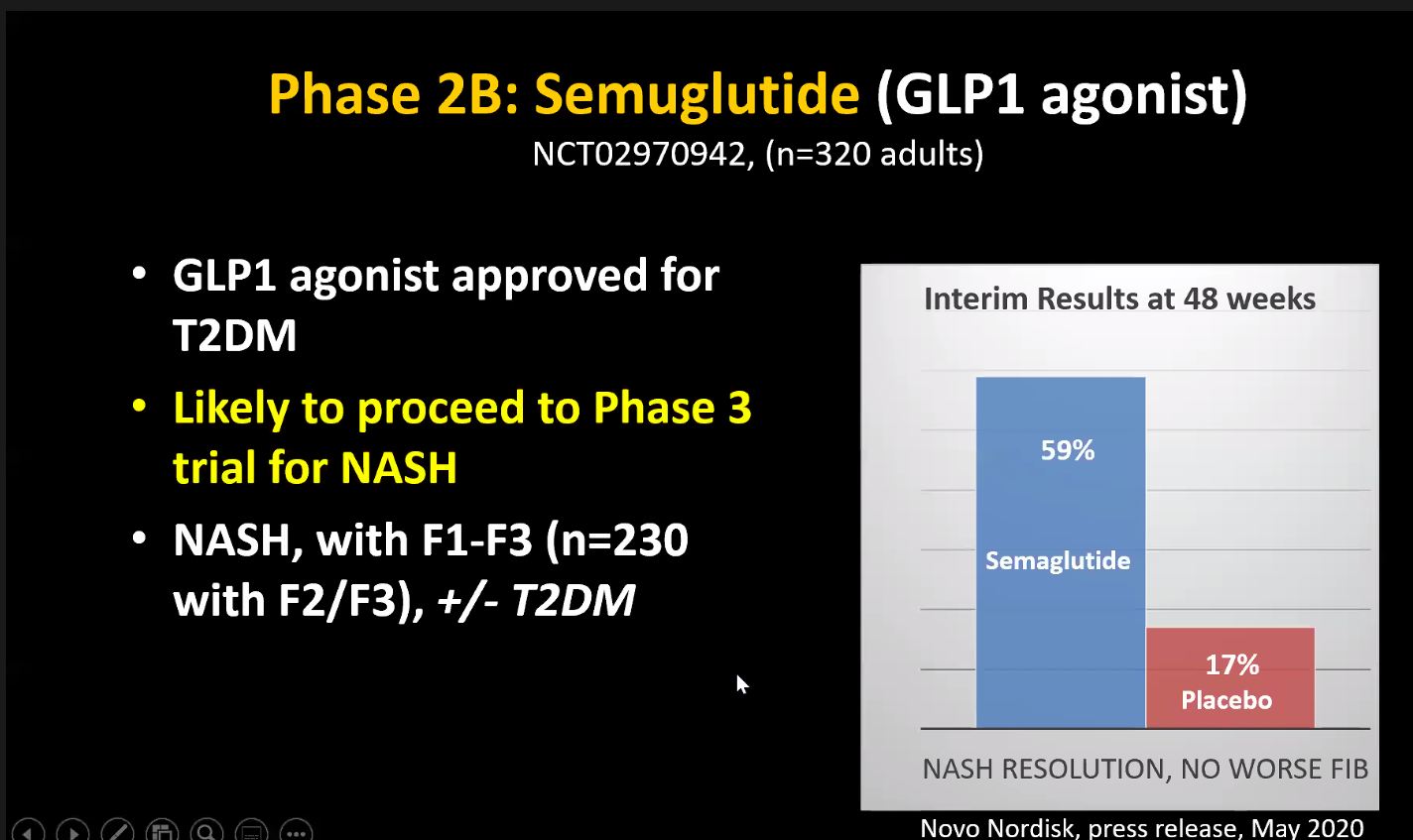
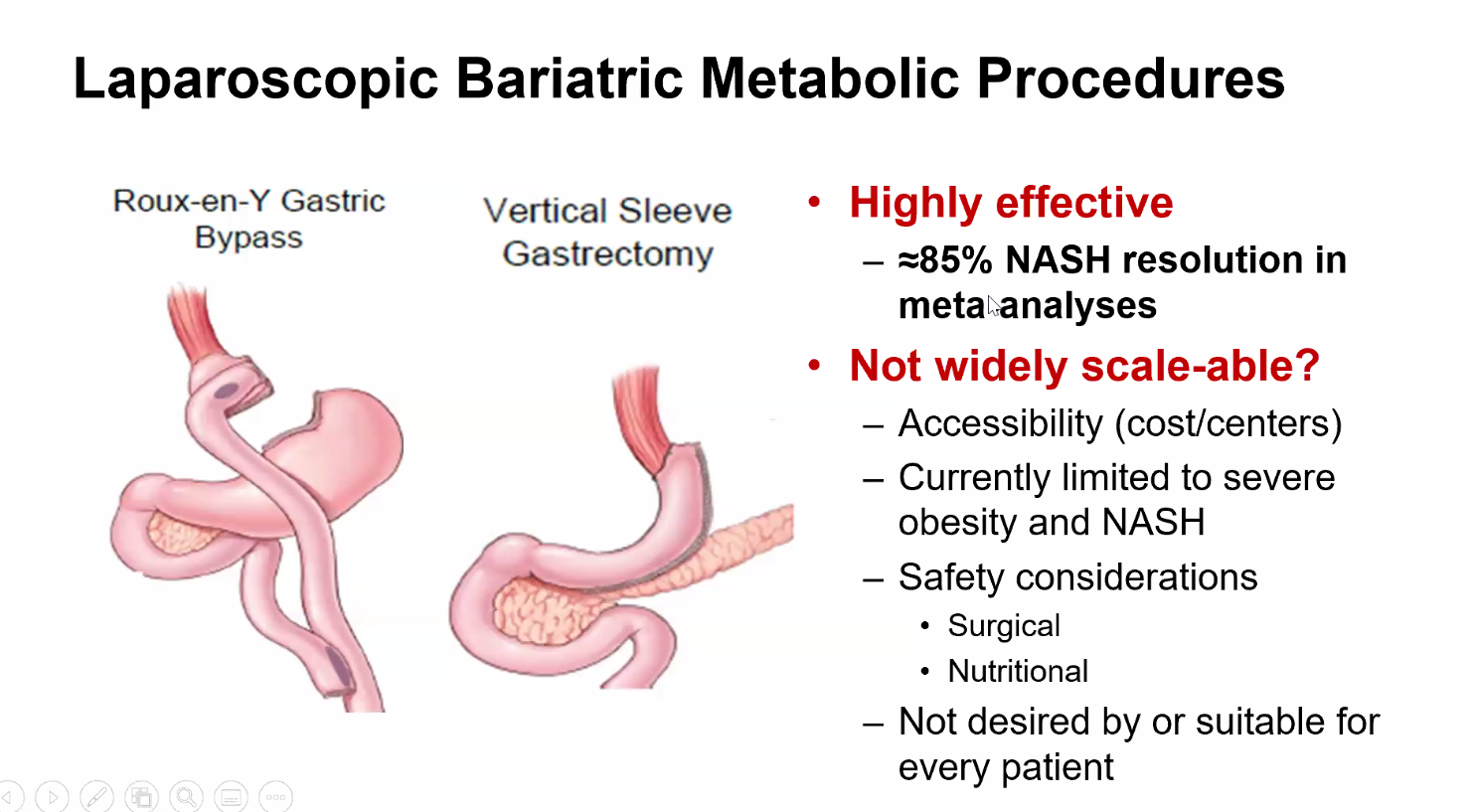
Discussed treatment, particularly diet and bariatric surgery. Stated that some emerging treatments look promising.
In those with suspected NAFLD, Dr. Xanthokos recommends liver biopsy, if lifestyle therapy is ineffective, under specific circumstances: prior to bariatric surgery, in some cases to determine severity, and prior to instituting therapy (eg Vitamin E)
A recent study (AJ Sanyal et al. Hepatology 2019; 70: 1913-27) used prospectively collected data from two large randomized, placebo-controlled phase 2b studies of simtuzumab in patients with either bridging fibrosis (n=217) or compensated cirrhosis (n=258) due to nonalcoholic fatty liver disease (NAFLD). The age range of participants were 48-61 years with median ages of 55 years and 57 years for the two cohorts. All patients had liver biopsies at screening and at weeks 48 and 96.
Key findings:
Progression to cirrhosis occurred in 22% (48/217) of patients with bridging fibrosis (F3) over a median of 29 months
Liver-related adverse clinical events (eg. ascites, variceal bleeding, encephalopathy, MELD score ≥15, liver transplantation or death) occurred in 19% (50/258) with compensated cirrhosis over a median of 29 months. Only 1 patient in this cohort died.
Higher baseline hepatic fibrosis or serum markers of fibrosis were associated with disease progression in patients with F3 disease
My take: Among those with advanced liver disease, this study indicates that disease progression/deterioration is rather rapid in about 20%.
E Cowell et al. JPGN 2019; 68: 695-99. This study reviewed 61 cases of pediatric hepatocellular carcinoma to determine predisposing conditions (in Houston TX). The majority did NOT have recognizable predisposing conditions. 25 of 61 (41%) had a predisposing condition including cryptogenic cirrhosis/steatosis (9), genetic (7), biliary pathology (4), viral hepatitis (1), and other (4). Those without a recognizable predisposing condition were diagnosed later and with more advanced disease/decreased survival.
VA McLin et al. JPGN 2019; 68: 615-22. Useful review on congenital portosystemic shunts.
DE Kaplan et al. Gastroenterol 2019; 156: 1693-1706. This large study form the VA with more than 70,000 patients examined the relationship between statin exposure and survival in patients with cirrhosis. “Each cumulative year of statin exposure was associated with an independent 8-8.7% decrease of mortality of patients with cirrhosis of Child-Turcotte-Pugh classes A and B.”
AG Singal et al. Gastroenterol 2019; 156: 1683-1692. Direct-acting antiviral therapy was not associated with recurrent hepatocellular carcinoma (HCC) in a multicenter cohort study with 793 patients with HCV-associated HCC. Thus, DAAs appear safe in patients who have achieved a complete response to HCC Rx
CL Mack et al. JPGN 2019; 68:495-501. This multicenter prospective open-label phase I/III trial of IVIG in biliary atresia patients status-post Kasai indicated that the infusions were tolerated. However, though this study was not powered to detect efficacy, survival with native liver was LOWER among patients who had received IVIG (n=29): 58.6% compared to the comparison placebo group 70.5% (n=64). Thus, despite the theoretical advantages of IVIG which targets aspects of the immune system and improvement in a murine model, in practice IVIG does not appear promising for biliary atresia.
D Kim et al. Hepatology 2019; 69: 1064-74. This study shows that despite improvements in hepatitis C mortality rates associated with newer treatments, there is an overall increase in mortality rates from cirrhosis and hepatocellular carcinoma. This increase is driven by increasing prevalence and severity of both alcoholic liver disease and nonalchoholic fatty liver disease. The overall cirrhosis-related mortality increased from 19.77/100,000 persons in 2007 to 23.67 in 2016 with an annual increase of 2.3%. Similarly, the overall HCC-related mortality increased from 3.48/100,000 persons in 2007 to 4.41 in 2016 at annual increase of 2%. The editorial on page 931 (TG Cotter and MR Charlton) notes that each year there are more than 40,000 deaaths associated with chronic liver disease.
H Park et al. Hepatology 2019; 69: 1032-45. This study, using Truven Health MarketScan Cata, examined the outcomes of more than 26,000 patients with newly-diagnosed hepatitis C virus (HCV) infection. Among the 30% who received oral direct-acting antiviral (DAA) therapy, there were improved outcomes in those with and without cirrhosis. In those with cirrhosis (n=2157), DAA was associated with a 72% and 62% lower incidences of HCC and DCC [decompensated cirrhosis] respectively. In noncirrhotic HCV patients (n=23,948), DAA was associated with a 57% and 58% lower incidence of HCC and DCC respectively. In addition to improved health outcomes, DAA treatment resulted in decrease health care costs, especially for patients with cirrhosis.
Z Kuloglu et al. JPGN 2019; 68: 371-6. In this multicenter Turkish study, the authors identified 810 children (median age 5.6 years) with unexplained transaminase elevation (62%),unexplained organomegaly (45%), obesity-unrelated liver steatosis (26%) and cryptogenic fibrosis or cirrhosis (6%). LAL-D [lysosomal acid lipase deficiency] activity was deficient in 2 siblings (0.2%); both had LDL ~155. Overall, even in at risk groups, LAL-D is rare.
Briefly noted: A recent study (NM Gorgis et al. Hepatology 2019; 69: 1206-18, editorial 940-2 by Elizabeth Rand) indicates that cirrhotic cardiomyopathy (CCM) is very important factor for survival for biliary atresia (BA) patients requiring liver transplantation.
CCM was defined based on two-dimensional echocardiographic criteria: LV mass index ≥95 g/meter-squared or relative wall LV thickness of LV ≥0.42.
Key points:
Overall, 11 of 69 patients died, 4 while awaiting liver transplantation and 7 following transplantation.
34 of 69 BA patients in this cohort had BA-CCM
All 11 who died had BA-CCM compared with no deaths in the 35 patients without CCM.
My take: Severe BA-CCM needs to be examined further; if severe, it may merit changing allocation policy.
Briefly noted: M Izzy, J Oh, KD Watt. Hepatology 2018; 68: 2008-2015. This concise review discusses the outcome of cirrhotic cardiomyopathy after liver transplantation.
Key point: “Although it is often believed that cirrhotic cardiomyopathy resolves post-LT, the data, albeit limited, do not support this postulation…diastolic function may not improve post-transplant and may actually worsen. Improvement in systolic function was suggested by only two of six studies.”
This figure from Hepatology November cover depicts a cirrhotic liver restricting the heart filling during diastole. (From Wiley Online Library -free access)
Despite widespread recommendations to screen patients with cirrhosis for hepatocellular carcinoma (HCC), a recent study (AM Moon et al. Gastroenterol 2018; 16: 1777-85) found “No Association Between Screening for Hepatocellular Carcinoma and Reduced Cancer-Related Mortality in Patients with Cirrhosis.” The title of the study did not make sense to me based on previous publications that have noted increased risk of HCC in patients with cirrhosis and the presumption that screening would allow effective interventions to prevent death due to HCC. So I looked at the study a little closer:
Background/Methods: The authors utilized a matched case-control study within the U.S. Veterans Affairs health care system to determine whether ultrasonography (US) or alpha-fetoprotein (AFP) screening was associated with decreased cancer-related mortality.
They identified 238 patients with cirrhosis who died of HCC between 2013-2015 –all of whom had a diagnosis of cirrhosis at least 4 years before the diagnosis of HCC. Then, they matched them with a control patient with cirrhosis who did not have HCC and had been identified at least 4 years prior to matched case’s HCC.
Key findings:
There was no significant difference between the cases and the controls in the proportions who underwent screening:
For U/S screening: 52.9% cases and 54.2% for controls.
For AFP (serum) screening, 74.8% vs 73.5% respectively.
For either U/S or AFP screening, 81.1% vs 79.4%.
For both U/S and AFP screening, 46.6% vs 48.3% respectively.
Table 4 provides odds ratios and adjusted odds ratios for the cases compared to controls. The Adjusted Odds ratios for U/S 0-4 years before index case was 0.95, for AFP 1.08, and for either U/S or AFP 1.11.
The authors found that HCC screening with U/S and/or AFP was not associated with decreased risk of HCC-related mortality.
In their study, the authors note that most studies on HCC screening have been observational which have numerous limitations including lead-time biases (which can overestimate the benefits of screening) and patient selection. Two randomized controlled trials reached conflicting conclusions; these trials were conducted in China where HCC is mainly associated with hepatitis B infection.
The authors point out that liver societies like AASLD and EASL have recommended U/S every 6 months with or without AFP measurements for HCC surveillance in patients with cirrhosis. However, non-liver societies have NOT “endorsed HCC screening because of the lack of high-quality data.” Neither the US Preventive Services Task Force nor the American Cancer Society make recommendations for HCC screening. And, “the National Cancer Institute found no evidence that screening decreases mortality from HCC but did find evidence that screening could result in harm.”
Strengths of this study:
All VA patients have access to medical care; this limits bias due to access to HCC screening
The matched-case control design with random controls across a system that delivers care to 8 million veterans across the country indicates that the findings are likely “typical of community-based settings” and likely to yield “estimates of the impact of screening …[that] approximates the results that would be expected from a randomized controlled trial”
Why Have Previous Studies Indicated that HCC Screening is Worthwhile?
According to the authors, even though HCC detected by screening is on average detected at an earlier stage than those detected due to symptoms, “this does not prove that screening leads to earlier detection. Another explanation is that screening is more likely to identify slow-growing tumors, which have a lower stage, and more likely to miss the fast-growing tumors, which are identified at a higher stage by symptoms.”
“It is possible that the HCCs most likely to lead to death are the HCCs least likely to be identified by current screening modalities at an early stage.”
In addition, “whether early treatment for HCC in patients with cirrhosis leads to a decrease in case fatality is questionable.” Patients who receive surgical resection or locoregional treatments remain at risk for recurrent HCC, new HCC and progressive liver dysfunction. While liver transplantation can cure HCC and cirrhosis, only a “small minority of patients with HCC undergo liver transplantation.” In 2012, only 1,733 patients received liver transplantation for HCC out of a reported 24,696 incident cases.
My take: This study offers a lot of insight regarding HCC screening and questions its usefulness, though I doubt this study will change how most hepatologists practice.