E Brindal et al. JAMA Netw Open. 2026;9;5):e2615637. doi:10.1001/jamanetworkopen.2026. 15637. Open Access! Regular Flatulence Patterns Among Community-Dwelling Individuals in Australia. Thanks to Stan Cohen for sharing this study.
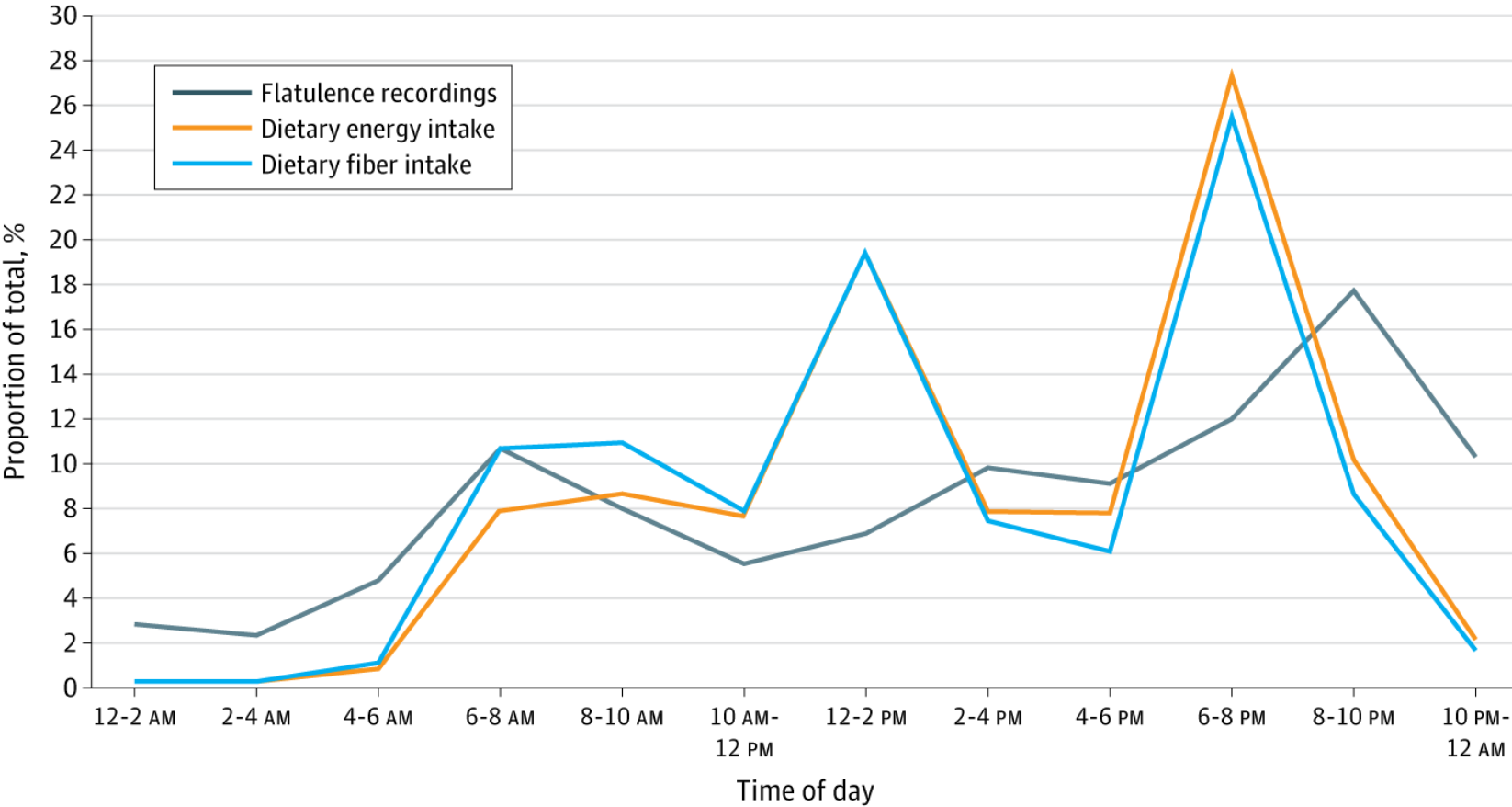
Methods: Cross-sectional study with 6416 participants Data were recorded into a purpose-designed mobile phone application (Chart Your Fart) by participants who logged their flatus passages in real time, consistent with experience sampling methods.3
Key findings:
- See Table below – Mean flatus per day was 5.0

Discussion:
- “In terms of range, observed data suggest good consistency with other methods, including retrospective frequency reports in a large US sample of individuals experiencing gas or bloating (n = 16 537),6 a small laboratory study that collected a median of 8 emissions throughout 24 hours,7 and even Benjamin Franklin’s personal account of “discharging wind from bowels” 7 times a day.8“
- “Limitations of this study include failing to quantify emissions made while asleep due to reliance on self-report.”
My take: Looks like another good study to discuss at the GI dinner table. Also, lots of jokes that would be apropos. Here’s one:
An elderly patient goes to her doctor and at the end of her exam she tells him there is one other matter that she would like to discuss. “It seems that I have frequent gas but fortunately it is silent and does not smell. I have even passed some gas while I’ve been here.” The physician says, “Hmmm… take these pills for one week and then come back.”
When she returns, she complains, “I don’t know what was in those pills. The gas now smells terrible but thank goodness it is silent.” The doctor replies, “Well, it looks like the antibiotics have improved your ability to smell. Now we need to get your hearing evaluated.”
Related blog post: Somewhat Funny Flatulent Research