R Rosen et al. Gastroenterol 2026; 170: 1347-1366. Open Access! Rome V Pediatric Upper Gastrointestinal Disorders of Gut-Brain Interaction
This article has a lot of useful information and I recommend reading the article in full. Yesterday’s post focused on Esophageal Disorders. Today’s reviews functional pediatric feeding disorders.
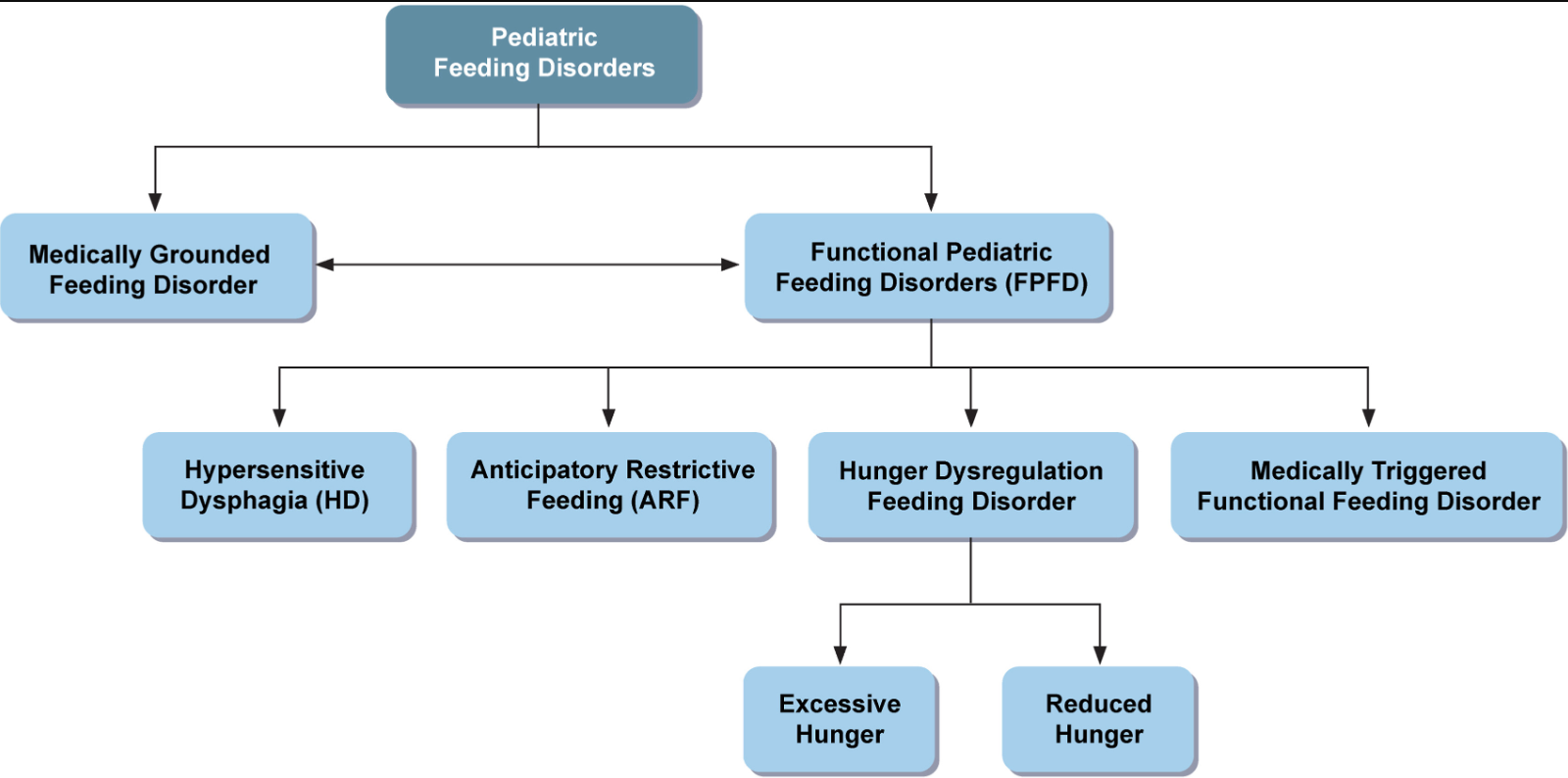
Functional Pediatric Feeding Disorders
- Hypersensitvie dysphagia
- Anticipatory Restrictive Feeding
- Hunger dysregulation feeding disorder
- Medically-triggered functional feeding disorder
The key points:
- “Pediatric feeding disorders affect 5%–20% of children and are associated with significant morbidity, decreased quality of life, and increased resource utilization.63,64“
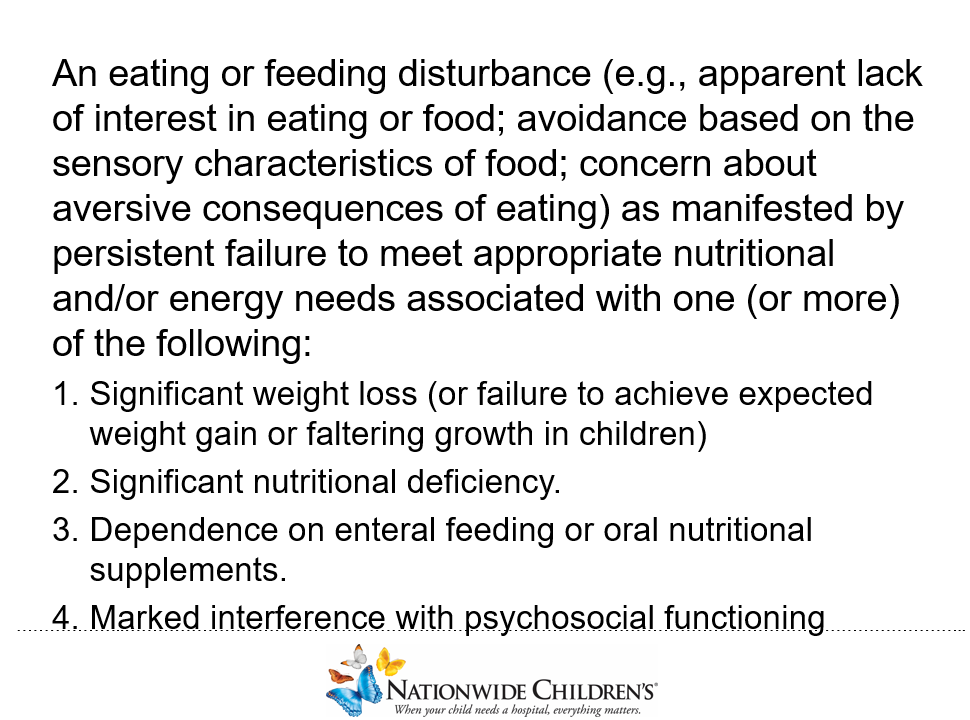
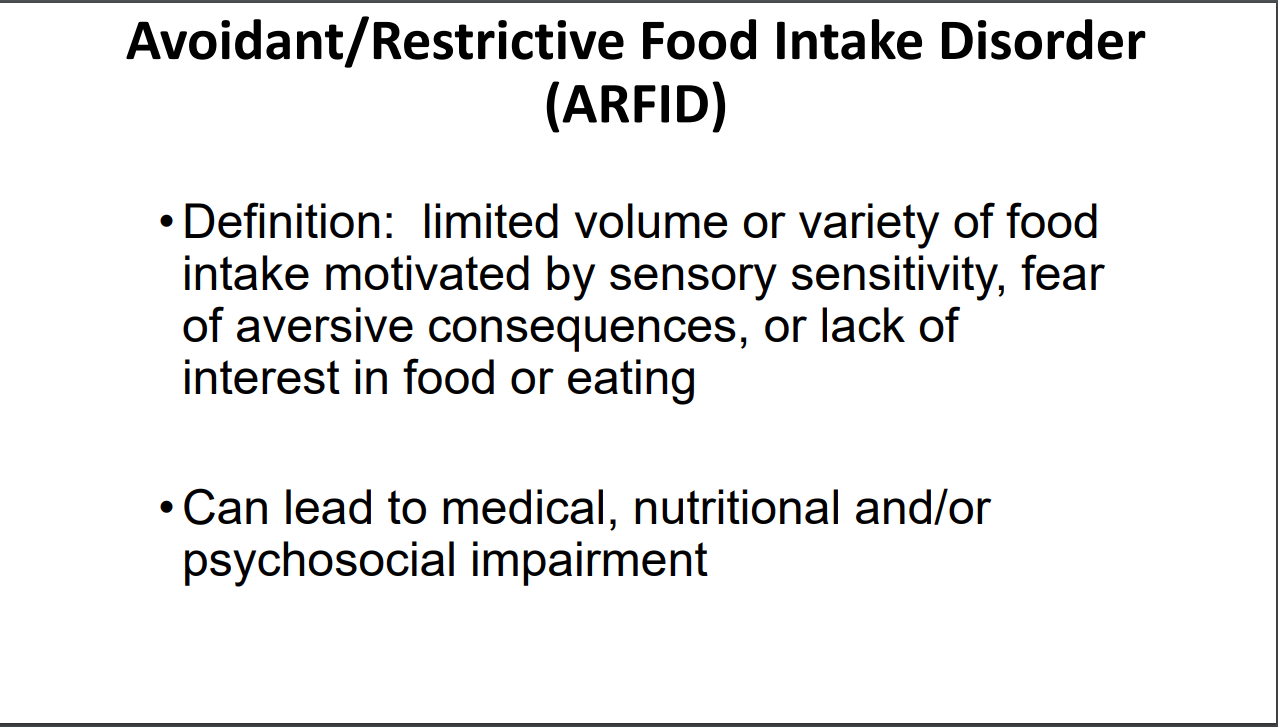
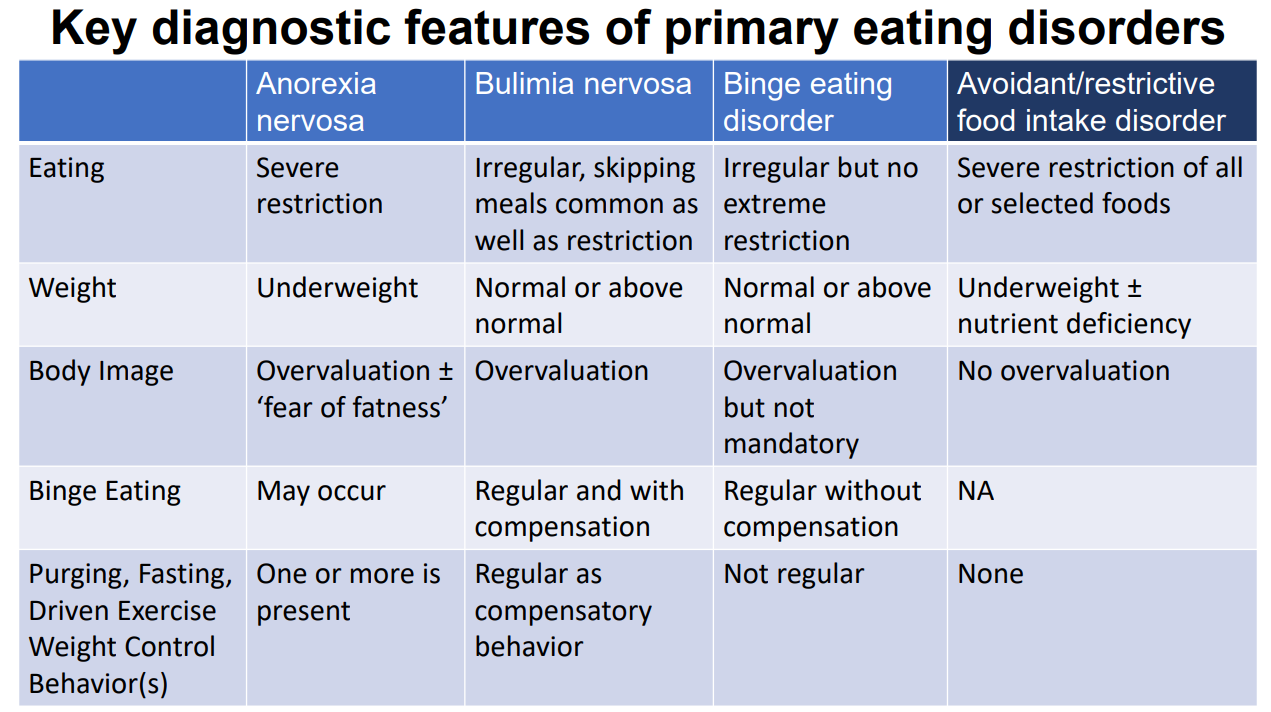
- “By merging examples of different feeding disorders under a single term, ARFID, the definition lacks needed granularity to refer patients for appropriate therapies. Therefore, we propose that the term ARFID should be eliminated and replaced by more precise terms.”
- “As these are new diagnoses, the relative proportions of subgroups are not known. In 1 study of children with ARFID, 43%–82% had a lack of interest in eating (the new “hunger dysregulation” diagnosis), 21%–68% had sensory-driven food refusal, and 11%–21% had swallowing difficulties (the new “hypersensitive dysphagia” [HD] diagnosis).67“
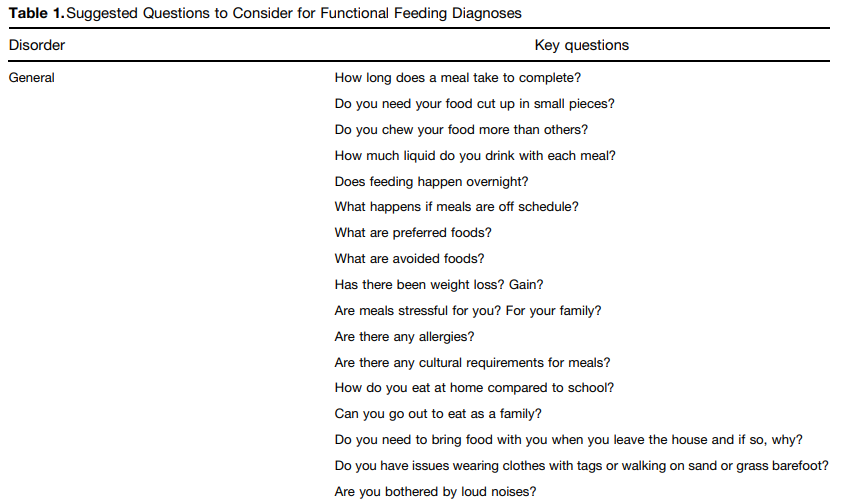
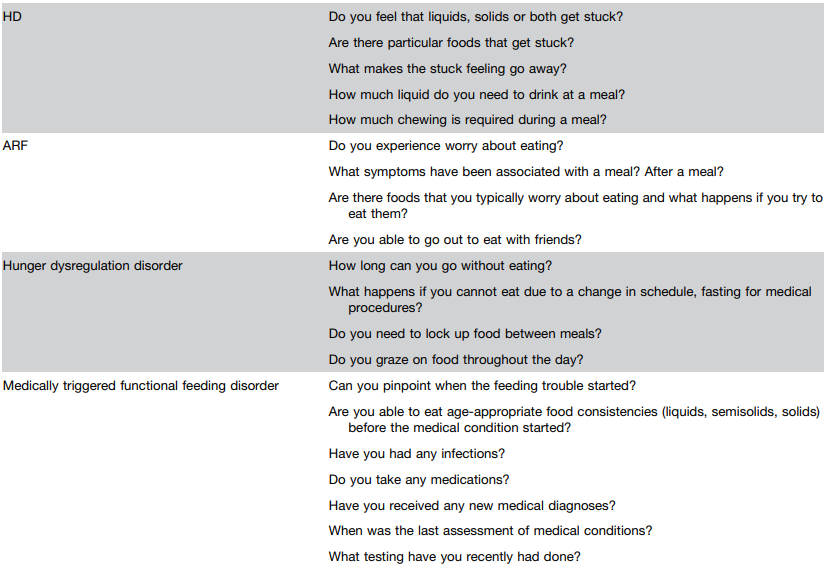
- “Children with HD [hypersensitive dysphagia] present with sensations of food feeling stuck despite normal esophageal anatomy, motor function, and bolus clearance.” This is similar to “functional dysphagia” in adults. However, HD includes both oropharyngeal and esophageal sensations because children cannot often differentiate locations or they will not put food in the mouth or will chew and spit food or drinks. Second, normal bolus transit (as measured by HRIM or esophagram if the former is not available) was added to the definition.”
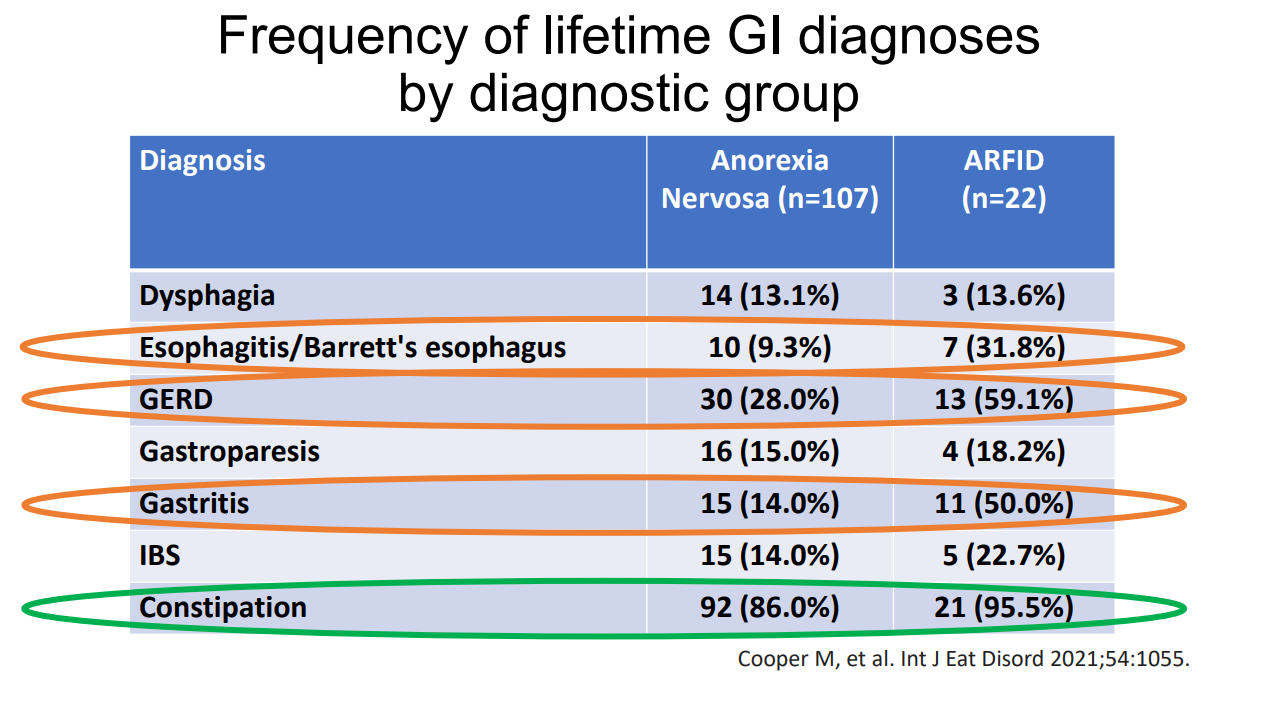
- “Anticipatory restrictive feeding (ARF) is characterized by the fear of an aversive experience with eating (eg, nausea, pain, bloating, gagging, choking, or vomiting). Clinically, these patients may present with significant diet restrictions resulting in elimination of entire food groups, specific food textures, or food temperatures. Children may express experiences of anxiety, disgust, or fear when consuming new, symptom-triggering, or nonpreferred foods…ARF is common in children with concurrent DGBI and the majority (>80%) of these patients have underlying GI symptoms.68,69“
- Testing: “Unlike many other DGBI, significant testing may be required before an FPFD diagnosis can be made because of the medical masqueraders (Figure 2) that may mimic an FPFD.73 Testing by feeding diagnosis is shown in Supplementary Table 2. Upper GI endoscopy is almost always recommended for pediatric feeding disorders because EoE can present with symptoms mimicking an FPFD; 25%–50% of patients with EoE have dysphagia and feeding issues and 15% of children with feeding issues have EoE.82–84 Laboratory testing for celiac disease, thyroid disease, a complete blood count, and electrolytes are indicated and, potentially expanded laboratory testing for iron, vitamin A, C, D, B12, carnitine, folate, liver function tests, thiamin, and zinc, depending on the history.83,85” The authors note that endoscopy is sometimes helpful for HD but is recommended in the other FPFD.
Treatments:
- “Restrictive diets such as the low fermentable oligo-saccharides, di-saccharides, mono-saccharides, and polyols diet, gluten-free diets, and dairy-free diets are not usually recommended for symptom control as they may increase meal-related anxiety, thus worsening or triggering an FPFD.86“
- “The majority of patients do not need enteral tube support. In the ARFID literature, 20%–46% of patients were reliant on some form of enteral support, although the approach to ARFID has recently moved away from enteral tube use toward multidisciplinary behavioral therapies.67“
- “Intravenous parenteral nutrition is not recommended for FPFD.”
- “For patients lacking a hunger drive, cyproheptadine has been found to increase appetite and improve gastric accommodation.87,88“
- “A retrospective review of intrapyloric botulinum toxin injections (IPBIs) in 85 young children with feeding disorders found some improvement with IPBIs.89“
Related blog posts:
- Mel Heyman: Past, Present and Future of ARFID
- Avoidant/Restrictive Food Intake Disorder (ARFID) with Irritable Bowel Syndrome and with Inflammatory Bowel Disease
- Risk of Eating Disorders with Dietary Therapy of Functional Abdominal Pain
- Dr. Praveen Goday: Tips on Managing Feeding Problems (Part 1)
- Dr. Praveen Goday: Tips on Managing Feeding Problems (Part 2)