In a previous post, I reviewed the 2025-2030 Dietary Guidelines for Americans (Have You Read the New “Dietary Guidelines for Americans, 2025-2030”?). For more insight into this topic, the following commentary is useful:
- DK Tobias, FB Hu. NEJM 2025; 394: 1969-1971. The 2025–2030 Dietary Guidelines for Americans — Progress, Pitfalls, and the Path Forward
Background: “The Dietary Guidelines for Americans (DGAs), updated every 5 years by the U.S. Department of Agriculture (USDA) and the Department of Health and Human Services (HHS), set nutrition standards for federally supported programs, including school, military, and institutional meals; elements of the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and the Supplemental Nutrition Assistance Program (SNAP); and related public education and implementation efforts. The DGAs also influence federal policies and regulations, clinical practice and health professional education, food marketing, industry formulation, and individual food choices.”
Key points:
- “In the current cycle, although the DGAC [Independent Dietary Guidelines Advisory Committee] rigorously adhered to established procedures,3 its extensive report was not adopted as the guidelines’ scientific basis, and only 14 of its 56 specific recommendations were implemented. The USDA and HHS cited the committee’s evaluation of the evidence “through a health equity lens” … as their central rationale for dismissing most of its recommendations.”
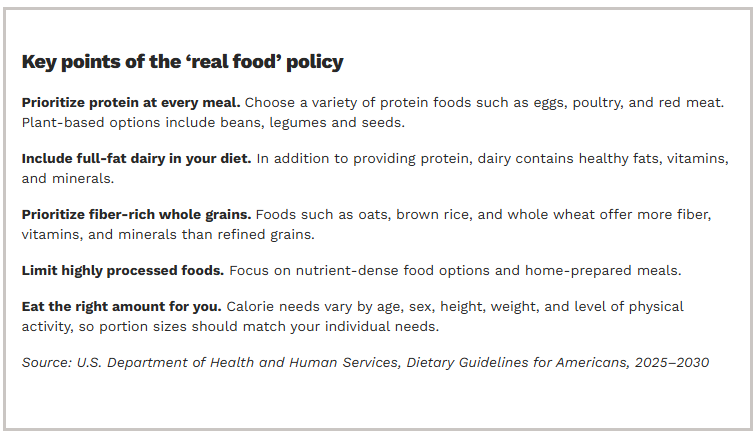
- “The new DGAs reintroduce the 1992 food pyramid, but invert it to feature meat, poultry, and full-fat dairy products more prominently, alongside vegetables and fruits, while relegating whole grains to the bottom wedge — an arrangement suggestive of a low-carbohydrate diet.”
- “The new DGAs increase recommended protein intake to 1.2-to-1.6 g per kilogram of body weight per day — as high as double the adult recommended dietary allowance (0.8 g per kilogram per day).4 … But most Americans already consume well above the recommended dietary allowance of protein, primarily from animal sources,3 and there is little evidence that substantially increasing population protein intake confers additional health benefits.”
- “The protein guidance appears to place greater visual and messaging emphasis on animal sources…This shift diverges from the broader scientific consensus, including the DGAC’s conclusion that dietary patterns higher in plant-derived proteins and fats, fruits, vegetables, and whole grains are associated with lower risks of chronic diseases, whereas higher intakes of red and processed meats are associated with increased risks.”
- “The 2025–2030 DGAs embrace concise, consumer-oriented messaging, emphasizing that Americans should “eat real food” and eat less highly processed food.1 Although this advice reflects growing concern about ultraprocessed products, its lack of specificity regarding ingredients or quantitative thresholds limits its policy relevance.”
- “Although the new DGAs continue to recommend limiting alcohol consumption, they no longer specify the quantitative upper limits included in previous guidelines, raising questions about the recommendations’ clarity and consistency.”
- “Restoring confidence in the DGAs will require stronger scientific grounding and greater transparency in their development.”
My take: Many of the recommendations appear to fall in line with previous viewpoints expressed by RFK Jr, regardless of what independent experts have advised. Overall, the new guidelines do not represent a significant improvement from the previous guidelines due to the problems outlined in this commentary.
Related blog posts:
- Have You Read the New “Dietary Guidelines for Americans, 2025-2030”?
- Humor: MAHAspital
- Is a High Protein Diet Beneficial and Safe?.
- “Optimal dietary patterns for healthy aging”
- “How to Make America Healthy: the Real Problems — and Best Fixes”
- “You Can’t Outrun a Bad Diet”
- NY Times: “Our Food is Killing Too Many of Us”