Methods: This study was a nationwide, population-based, matched cohort study using the Epidemiology Strengthened by Histopathology Reports in Sweden (ESPRESSO) cohort which included all adults in Sweden with incident achalasia (n = 704; 1969–2017; follow-up until December 31, 2021) without any other prior esophageal conditions. Individuals with achalasia were matched by age, sex, birth year, and county to up to 5 reference individuals (n = 3348) from the general population. The median follow-up was 9.1 years. Medians age in the study was 60 years.
Key findings:
There were 270 deaths in individuals with achalasia, and 1023 in reference individuals (IR, 69.4 vs 51.9/1000 person-years)
Thus, there was a 42% increase in the risk of death. This translated into 1 extra death per every 6 individuals with achalasia followed for 10 years
Risk increases were seen for death from any cancer (aHR, 1.65), esophageal cancer (aHR, 23.19), and respiratory disease (aHR, 2.22)
Discussion point: “The sibling comparison (aHR for all-cause mortality, 1.78; 95% CI, 1.13–2.81) confirmed our findings in the main analysis (aHR, 1.42; 95% CI, 1.21–1.65). The similar risk estimates suggest that shared early-life exposures do not play any major role for mortality in achalasia. In all, we are confident that the observed elevated mortality is unlikely to be fully explained by environmental exposures or comorbidities, because the risk estimates remained largely unchanged in the sibling comparison as well as after adjustment for a wide range of comorbidities (through CCI).”
My take: This study is in agreement with others which have sown that achalasia is associated with an increased mortality risk.
This prospective multicenter study included 384 patients with a mean age of 30 years (34% pediatric).
Key findings:
Daily abdominal pain decreased from 65% to 23%, whereas the mean pain score decreased from 4.9 (SD, 2.3) to 2.3 (SD, 2.5; both P < .001)
Opioid use decreased (assessed over a 14-day interval) from 61% before to 24% at 1 year after TPIAT (P < .001)
Improved physical and mental health: Physical component summary and mental component summary scores improved by ≥10 points in 58% and 35%, respectively
Mean hemoglobin A1c was 7% (SD, 1.9%) with 20% insulin independent at 1 year
Young age was associated with better outcomes, whereas duration and etiology of disease did not predict response to TPIAT
In their discussion, the authors note that it had been “widely hypothesized that after several years of pain, mechanism shift to solely neuropathic pain, such that surgery would be unlikely to offer benefit. Our results suggest this is not true.”
My take: This study provides robust data supporting TPIAT as average pain scores declined by more than 50%, the need for opioid analgesics decreased substantially, and mental health/physical health/QOL all improved. Most maintained glycemic control.
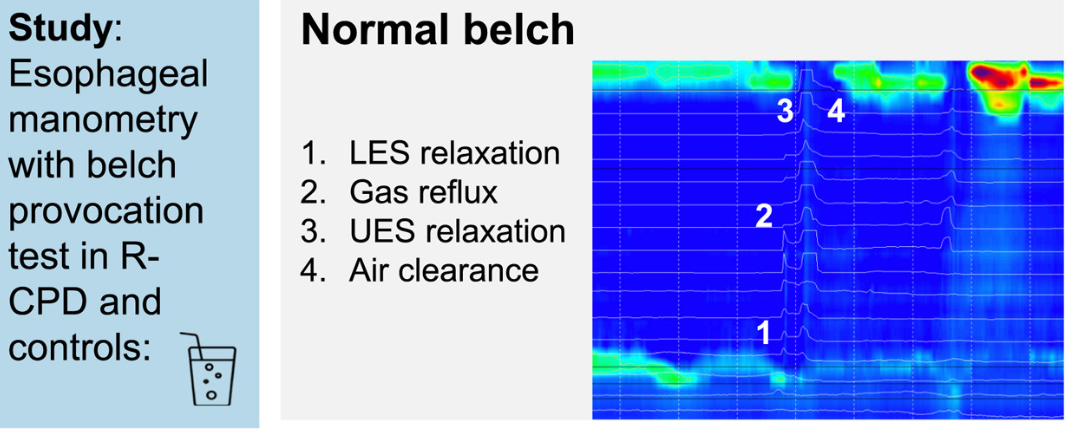
Methods: Retrospective analysis of High Resolution Impedance Manometry (HRiM) with belch provocation was performed between May 2021 and April 2024 in 55 patients with R-CPD, 30 control patients, and 15 healthy volunteers. Age of patients with R-CPD was 22-35 years.
Key findings:
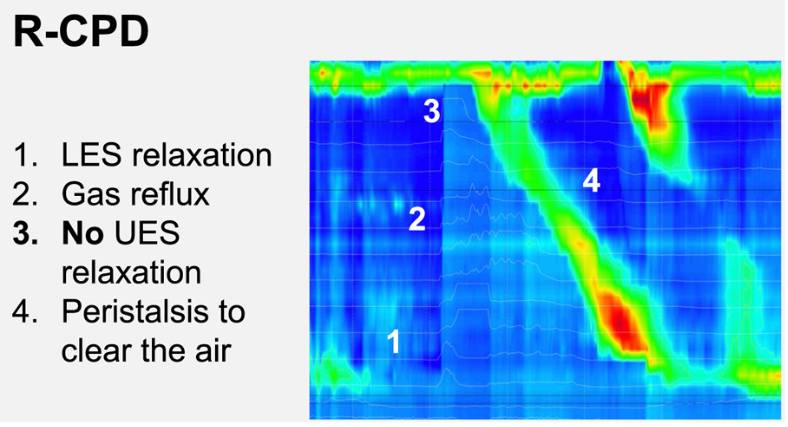
During belching, we saw higher UES pressures in R-CPD patients vs controls, leading to incomplete air clearance and air oscillating in the esophagus (P < .0001)
After BT injection, median UES pressures during belching decreased (56 vs 3 mmHg), and air clearance improved (P < .0001)
A maximum UES pressure during belching >31 mmHg adequately discriminated patients from controls
Interestingly, the authors did not include one of the major findings in their abstract: “Symptom improvement of at least 50% was present in 57% of patients, which is lower than reported up to now”
R-CPD patients had inability to belch in 100%, gurgling chest noises in 100%, bloating in 92%, chest pain in 67%, nausea in 59%, and heartburn (at least weekly) in 65%
My take: Recognition of this treatable disorder is important. However, the lower improvement rate in this study is useful for counseling patients. My suspicion is that this finding likely reflects more widespread results as initial studies could have more selection or reporting bias.
B Kang et al. Clinical Gastroenterology and Hepatology; 2026: 24: 201 – 209. Proactive Drug Monitoring Versus Clinically Based Dosing for Endoscopic Healing in Pediatric Crohn’s Disease Receiving Infliximab
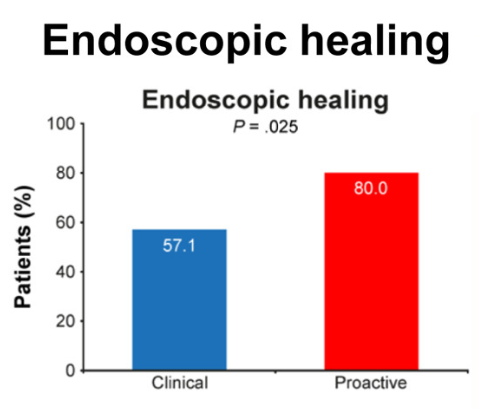
Methods: This was a non-blinded, randomized controlled trial of 112 biologic-naïve children with CD who had responded to IFX induction treatment at 4 centers in South Korea between July 2017 and November 2020. Patients were randomly assigned to receive dosing based on proactive TDM (proactive arm) or clinically based dosing (clinical arm). The primary endpoint was endoscopic healing (EH) at week 54.
During the maintenance phase, patients received IFX 5 mg/kg every 8 weeks. In the proactive arm, treatment was intensified (shortening interval by 2- to 4-weeks) if trough level was less than 6 mcg/mL.
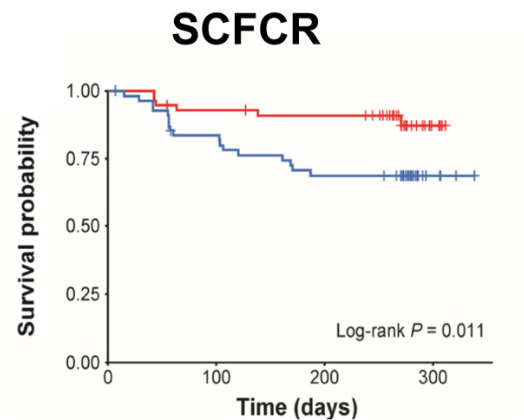
“Our findings provide evidence that the proactive strategy resulted in increased EH rates and had a positive impact on SCFCR, biochemical remission, and FC, which serve as surrogate markers of EH.”
“The PAILOT trial, the only prospective study on proactive TDM in pediatric patients with CD, demonstrated that proactive TDM with adalimumab resulted in higher SCFCR rates than reactive TDM (82% vs 46%; P < .001), consistent with our findings.8“
“In our study, IMM [immunomodulator] modulation was performed in conjunction with proactive TDM, which may explain why no difference was observed in ADA development (proactive arm, 31.4% vs clinical arm, 28.6%. Proactive TDM has been confirmed to reduce the development of ADAs, and the concept of “optimized monotherapy” based on the view that proactive TDM effectively guides IMM withdrawal in combination therapy has been well-described.30 …in our institution, IMMs are discontinued as soon as possible after 1 year of combination therapy if adequate TDM is maintained.31“
My take: This study shows that proactive TDM is superior to clinical-based dosing. The findings may have been less pronounced if higher baseline doses of IFX were used. It is well-recognized that “standard” IFX (5 mg/kg/dose every 8 weeks) is usually insufficient in pediatric patients.
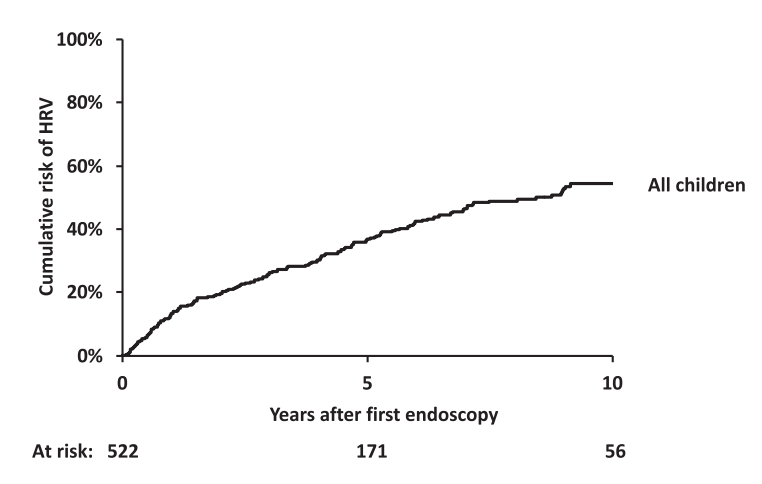
O Ackermann et al. Gastroenterol 2026; 170: 188-198. The Natural History of Gastroesophageal Varices in Children With Portal Hypertension
Methods: Retrospective review of 1586 children with portal hypertension. 590 had two or more upper endoscopies (403 with biliary atresia).
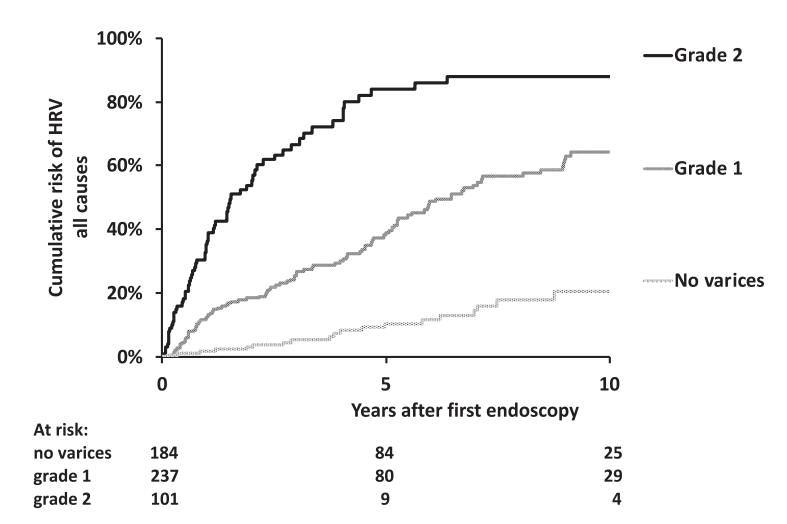
“For the purpose of this study, and based on our previous experience in children,8,11 the endoscopic pattern associated with a high risk of bleeding (ie., HRV) included grade 3 esophageal varices as well as grade 2 esophageal varices with red color signs or gastric varices (cardia), or both.”
The authors developed a HRV [high risk of varices] score as a composite index calculated as follows: 1 point for grade 1 esophageal varices, 2 points for grade 2 varices, 3 points for grade 3 varices, and 1 point each for the presence of red color signs or GOV1 (HRV score range, 0–5). High-risk varices had an HRV score of 3 to 5.
Key findings:
Worsening of the endoscopic pattern occurred in 58% of children over a mean 4-year interval
5- and 10-year probabilities of HRV emergence in initially HRV-negative children were 36% and 54%, respectively
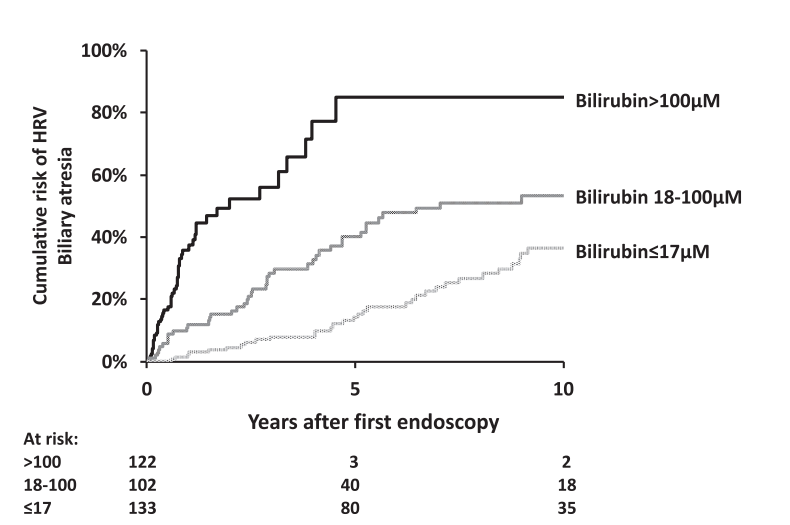
Infants with biliary atresia are at particularly high risk with correlation to the degree of cholestasis (see below)
Platelet count less than 150,000 as an indicator of HRV was mainly useful in older children. “A platelet count of ≥150,000/mm3 was recorded in 205 of the 629 children (32%) with HRV. Moreover, there was a decrease with age in the proportion of children with HRV and a platelet count of ≥150,000/mm3, falling from 62% in children aged <12 months to 2% in patients aged >10 year.” 16% of children 6-8 yrs, 12% of children 8-10 years of age with HRV had platelet count ≥150,000/mm3
“Gastrointestinal bleeding was recorded in 36 of 947 children (3.8%) who did not have HRV at their last endoscopy and in 270 of the 359 children (75%) with HRV at their last endoscopy who did not undergo endoscopic or surgical primary prophylaxis of bleeding.”
Bilirubin of 100 micoMol is equivalent to 5.8 mg/dL and 17.1 is eqivalent to 1 mg/dL
Discussion Points:
Variceal progression was much faster in infants and is is likely due to the severity of cholestasis and its impact on portal hypertension.
“It is notable that children with Alagille syndrome and those with genetic cholestasis with normal GGT have a lower rate of variceal progression and a lower mean HRV score than children with biliary atresia, despite comparably high levels of bilirubin. This suggests that different mechanisms of cholestasis … may have distinct consequences on intrahepatic portal vein branches resulting in varying degrees of portal hypertension.”
“In children with biliary atresia aged <12 months, grade 2 esophageal varices without red color signs or GOV1 (HRV score of 2) should be considered an indication for endoscopic primary prophylaxis.”
“Because the efficacy and safety of β-blockers have not been established in children, we suggest that this pattern—grade 1 varices with red color signs or GOV1—should prompt early repeat endoscopy to detect HRV in a timely manner…this repeat endoscopy could be recommended 6 months after the previous one.”
Limitations: High proportion of children with biliary atresia (limits conclusions with other disorders), and retrospective study since 1990
“Pending the results of future studies, the detection of palpable splenomegaly remains a simple and practical criterion for initiating screening endoscopy in children with portal hypertension”
My take: This is a very useful study providing important data to help improve decision-making in children with portal hypertension.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
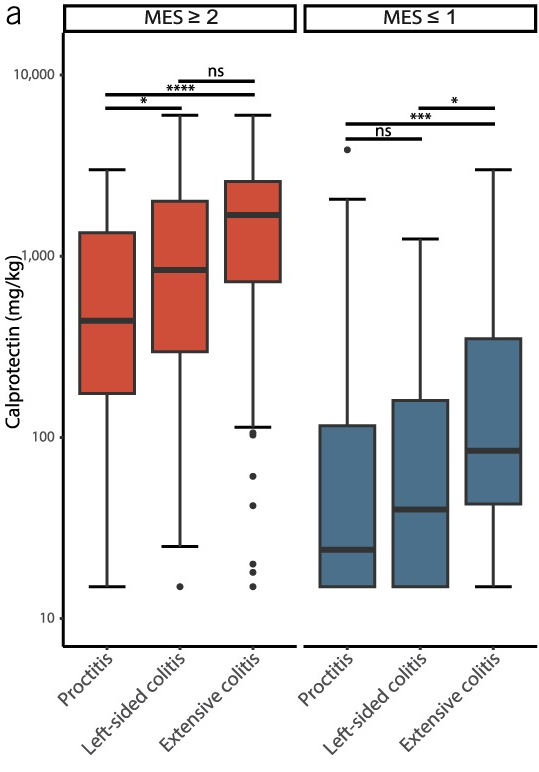
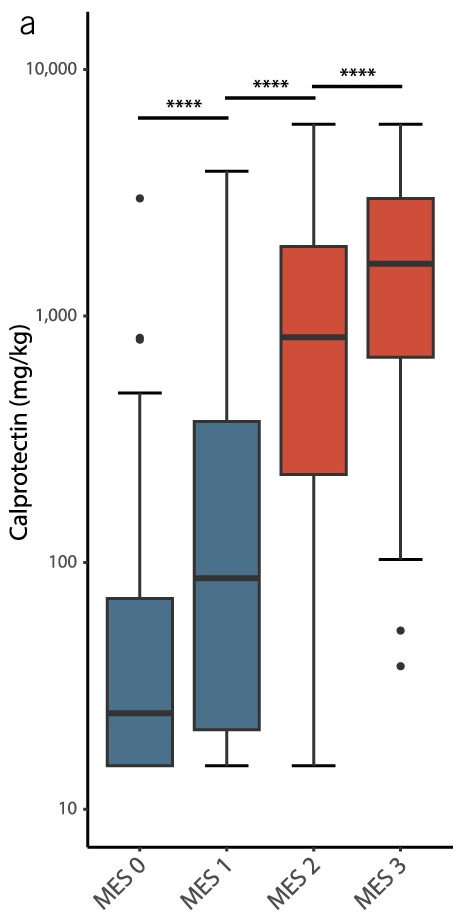
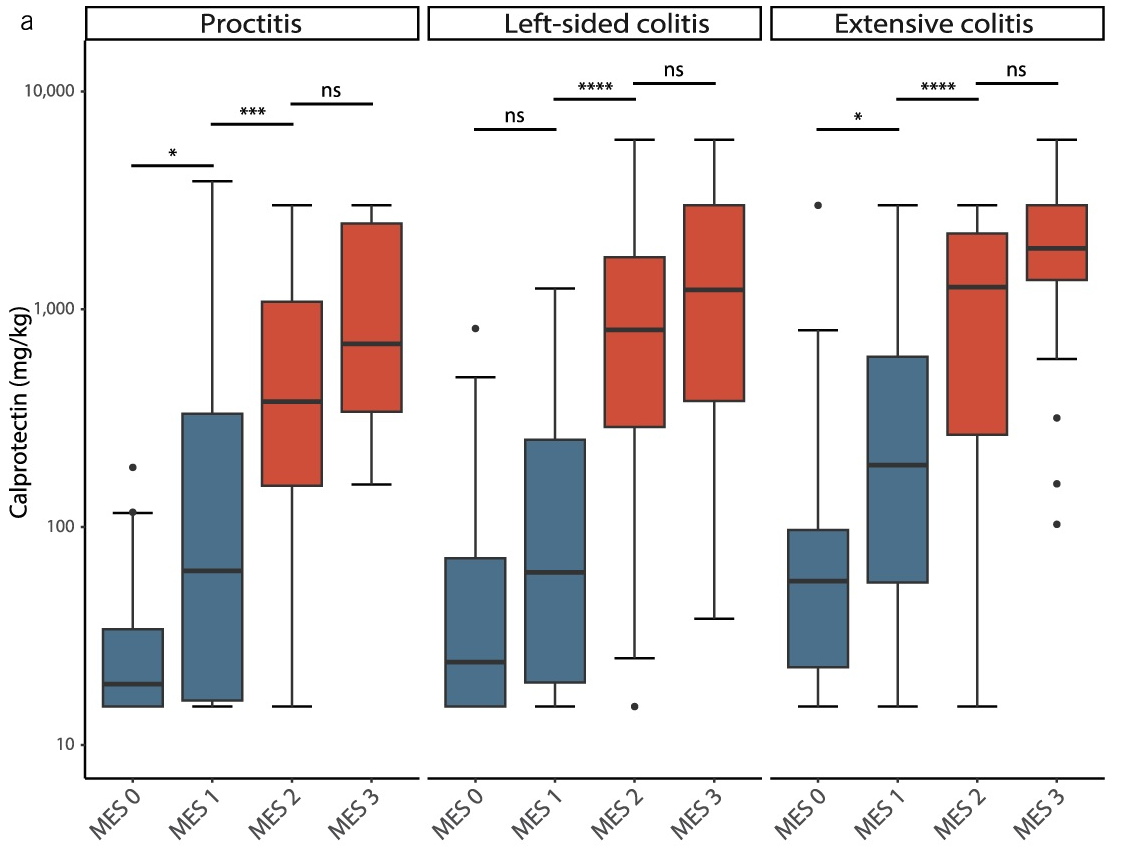
This single-center observational study (n=254) examined the correlation between fecal calprotectin (FC) levels with both disease extent and mucosal healing in ulcerative colitis. Mucosal healing was rated by the Mayo Endoscopic Score (MES).
Key findings:
Disease extent: FC levels were significantly lower in proctitis (440 mg/kg) as compared with left-sided colitis (840 mg/kg) or pancolitis (1,690 mg/kg)
Mucosal healing: In MES ≤1, FC levels were significantly lower in proctitis (24) compared to left-sided colitis (40) or pancolitis (85)
My take: Fecal calprotectin levels are clearly affected by the extent of disease involvement. However, the increase in calprotectin values associated with disease activity was significantly larger than the differences attributed to disease extent.
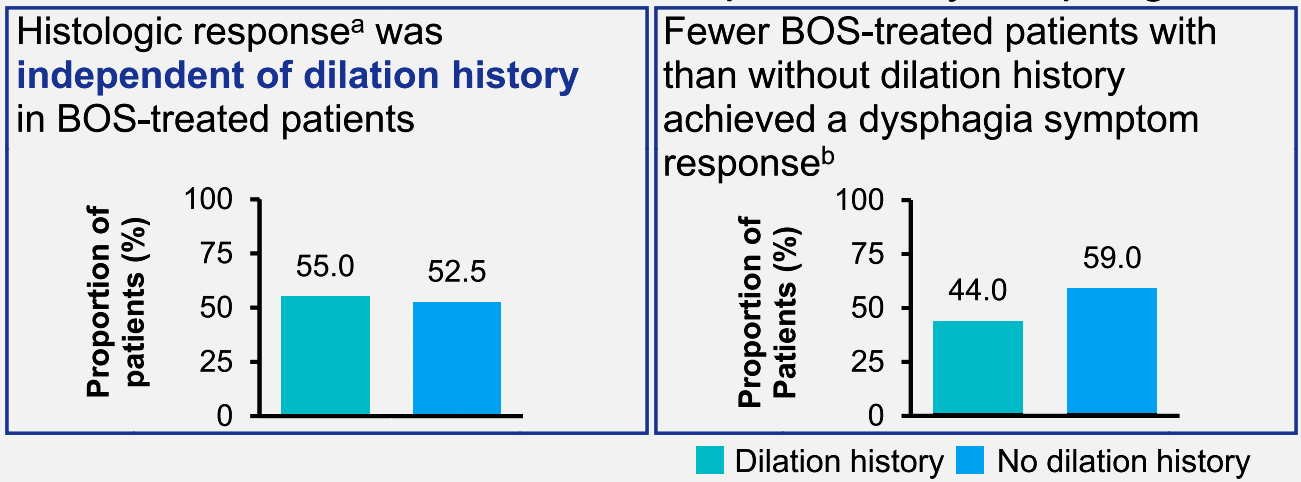
Methods: This post hoc analysis assessed data from a 12-week, randomized, double-blind, placebo-controlled phase 3 study (NCT02605837) of budesonide oral suspension (BOS) 2.0 mg twice daily in patients (n=318) aged 11–55 years with EoE and dysphagia. Coprimary efficacy outcomes were histologic (≤ 6 eosinophils per high-power field [eos/hpf]) and dysphagia symptom (≥ 30% reduction in Dysphagia Symptom Questionnaire scores from baseline) responses at week 12.
Key findings:
Histologic responses (≤ 6 and < 15 eos/hpf) were similar regardless of dilation history
Fewer BOS-treated patients with dilation history than no dilation history achieved a dysphagia symptom response (44.0% vs 59.0%)
Discussion Points:
“Esophageal dilation may provide immediate relief from dysphagia (15); symptom improvement has been observed in 95% of dilated patients with EoE (29)…[however] dilation does not affect the underlying inflammation (18).”
“A histologic response (<15 eos/hpf) to swallowed corticosteroids has also been associated with a reduced number of repeat esophageal dilations required to maintain a similar esophageal caliber compared with nonresponse (≥15 eos/hpf)…this supports swallowed corticosteroid use in patients who have undergone esophageal dilation, even in the absence of acute symptom improvement.”
“Study limitations include potential enrollment of patients with severe disease due to stringent inclusion criteria.”
My take: While dilatation alone often improves symptoms, treatment with budesonide may help reduce need for repeat dilatations.
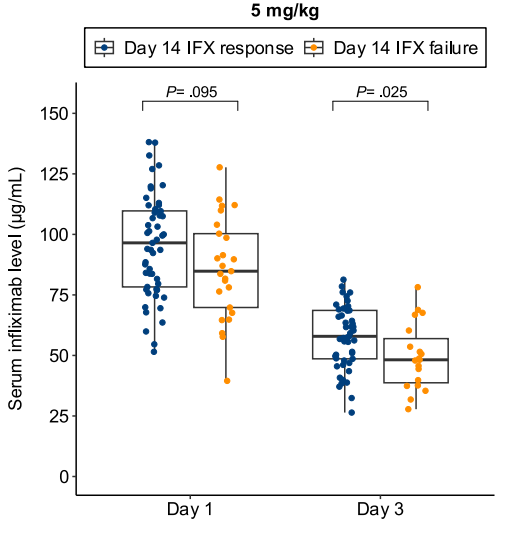
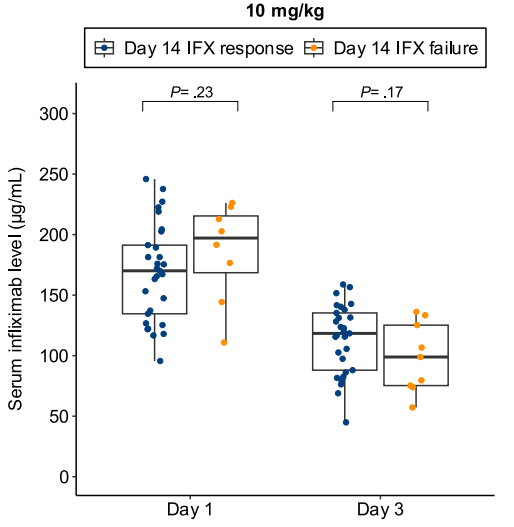
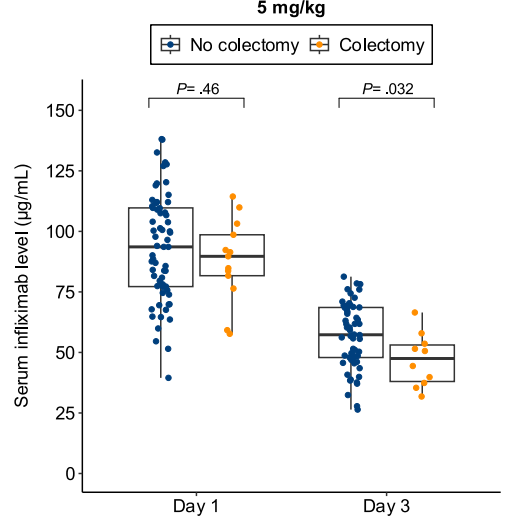
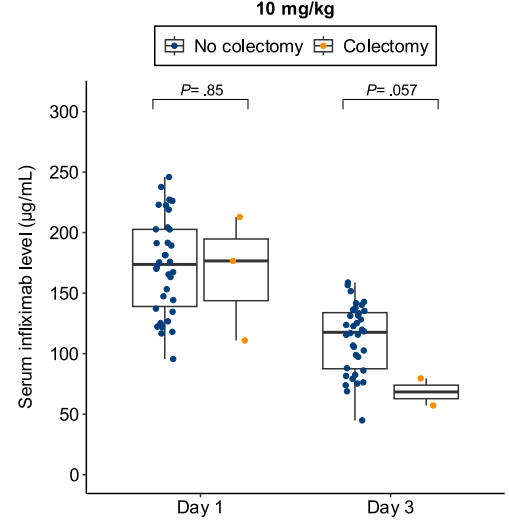
CFD Li Wai Suen et al.Gastroenterology, Volume 170, Issue 1, 118 – 131. Early Infliximab Levels and Clearance Predict Outcomes After Infliximab Rescue in Acute Severe Ulcerative Colitis: Results From PREDICT-UC
Methods: Data, including serum and stool testing, was extracted from from 135 patients (ages 24-42) enrolled in the PREDICT-UC prospective, randomized controlled trial
Key findings:
Lower day 3 serum infliximab levels predicted infliximab failure on day 14 and colectomy by 3 months; a threshold of ≤57.9 μg/mL had 83% sensitivity, 67% specificity, 24% positive predictive value, and 97% negative predictive value for colectomy
In patients with high clearance who did not respond to the first infliximab dose, day 14 response rate was higher with a second 10 mg/kg vs 5 mg/kg dose (38% vs 11%; risk ratio, 3.43)
Day 3 fecal infliximab levels correlated with endoscopic severity and was associated with day 7 nonresponse (P = .016)
Discussion points:
“Early infliximab levels and clearance predict outcomes in ASUC. Additionally, we are the first to demonstrate that a high early infliximab clearance can be overcome by additional dosing. These results demonstrate the potential of early infliximab TDM [therapeutic drug monitoring] to guide decision-making in ASUC and for the first time provide an evidence base for intensified infliximab dosing in clinical practice.”
My take: While the authors suggest TDM as a potential strategy to overcome low levels, an alternative approach would be using higher dosing and more frequent dosing, especially as infliximab levels may not be quickly available. Higher dosing is particularly important in the pediatric age group where studies have shown that “standard” dosing of 5 mg/kg result in insufficient levels of infliximab in ~80%.
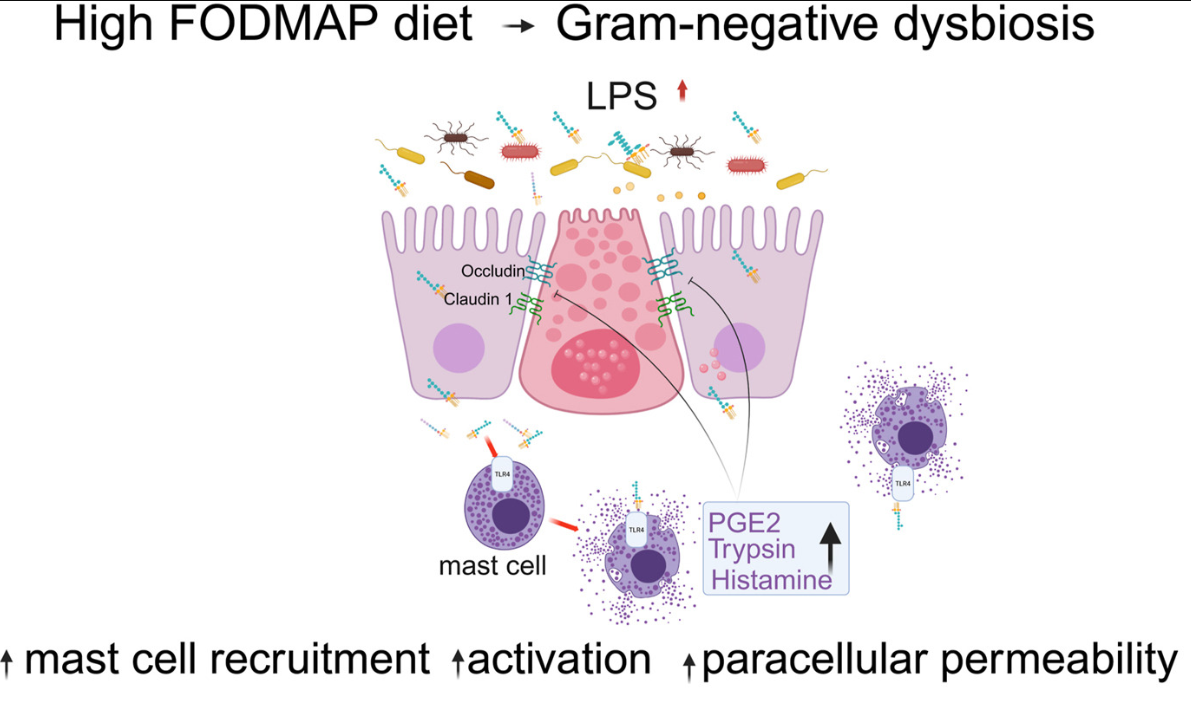
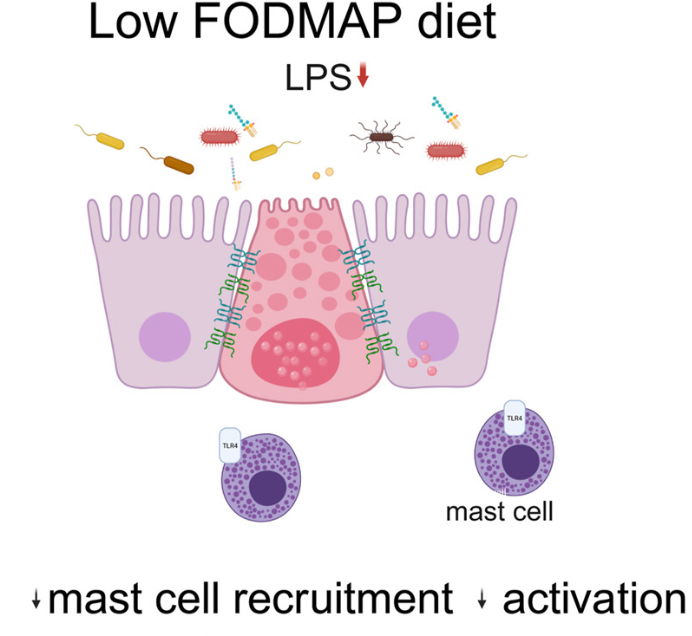
Background: “Mechanisms by which fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) drive pathophysiology of irritable bowel syndrome (IBS) are not well understood.”
Methods: 42 patients with “Rome IV diarrhea-predominant IBS (IBS-D) underwent barrier function evaluation pre- and post-LFD along with assessment of mast cell number and activation profile. Finally, fecal supernatants (FS) were administered intracolonically to wild-type mice with and without pharmacologic inhibition, toll-like receptor 4 (tlr4)–/– mice, and mast cell-deficient mice with/without mast cell reconstitution.”
Key findings:
This is a highly technical study and would recommend reviewing the findings directly (open access article).
To summarize:
“Patients with IBS-D had significant improvement in colonic barrier structure and function, mast cell number, and levels of mast cell mediators post-LFD (low FODMAP diet). The magnitude of physiological changes did not correlate with the magnitude of clinical response.”
“This study showed the complex interplay among food, microbiome, local immune activation, and epithelial physiology in IBS by demonstrating that FODMAPs increase fecal lipopolysaccharide levels, which activates colonic mast cells to causes barrier dysfunction in diarrhea-predominant IBS.”
My take: By understanding the GI effects of a low FODMAP diet in patients with IBS-D more precisely, it may improve dietary approaches as well as other treatments like mast cell stabilizers.
Background: “Obesity has historically been defined using body mass index (BMI). However, BMI does not account for adipose tissue, limiting its accuracy. The Lancet Diabetes & Endocrinology Commission created a revised obesity definition including anthropometric measures (waist circumference [WC], waist-to-hip ratio [WHR], and waist-to-height ratio [WHtR]),1 encompassing and subcategorizing preclinical obesity (excess adiposity without organ dysfunction or physical impairment) and clinical obesity (a disease).”
Methods: The authors analyzed 14,414 participants representing 237,700,000 US adults. using the 2017-2023 National Health and Nutrition Examination Survey (NHANES)
Key findings:
Survey-weighted obesity prevalence was 75.2%
Obesity was noted in 100% among adults with BMI of 30 or greater, 80.4% with BMI 25 to less than 30, and 38.5% with BMI less than 25
Discussion Points:
“These findings demonstrate the impact of anthropometric thresholds, particularly since 80.0% of adults had waist-to-height ratio [WHtR]) above 0.5. Though this value was cited by the Lancet Commission and identifies cardiometabolic risk,1,4,5 the commission emphasized that additional research was required for this cutoff.1“
My take: This is a provocative study indicating that even more U.S. adults could be considered obese when incorporating anthropometric criteria. More data is needed to assess the outcomes of this group that is considered obese with new criteria but not by using BMI criteria.
BAPS (Bochasanwasi Akshar Purushottam Swaminarayan Sanstha) Atlanta. This is a magnificent Hindu spiritual center in Lilburn. No photos are allowed inside though there are several online (see below).