Recent pediatric Rome V recommendations suggested the use of CYP2C19 testing in patients with reflux that was not responding to time-limited therapy (link: Rome V Pediatric Upper Gastrointestinal Disorders of Gut-Brain Interaction (Part 1)). The following retrospective study of adults (n=421) at an academic medical center provides a strong rationale.
L Creech et al. Clin Gastroenterol Hepatol 2026; 24: 1550-1557. Open Access! High Prevalence of CYP2C19 Rapid and Ultrarapid Metabolism Among Patients With Gastroesophageal Reflux Disease
Key finding:
- 44% (n=184) of patients presenting to gastroenterology clinic with gastroesophageal reflux disease who underwent CYP2C19 genotyping were found to be rapid metabolizers (RMs) (38%) or ultrarapid metabolizers (6%)
- The prevalence of Barrett’s esophagus/erosive esophagitis was higher among ultrarapid metabolizers (24%; n = 5/21) than among normal metabolizers (7%; n = 12/165; odds ratio, 3.5)
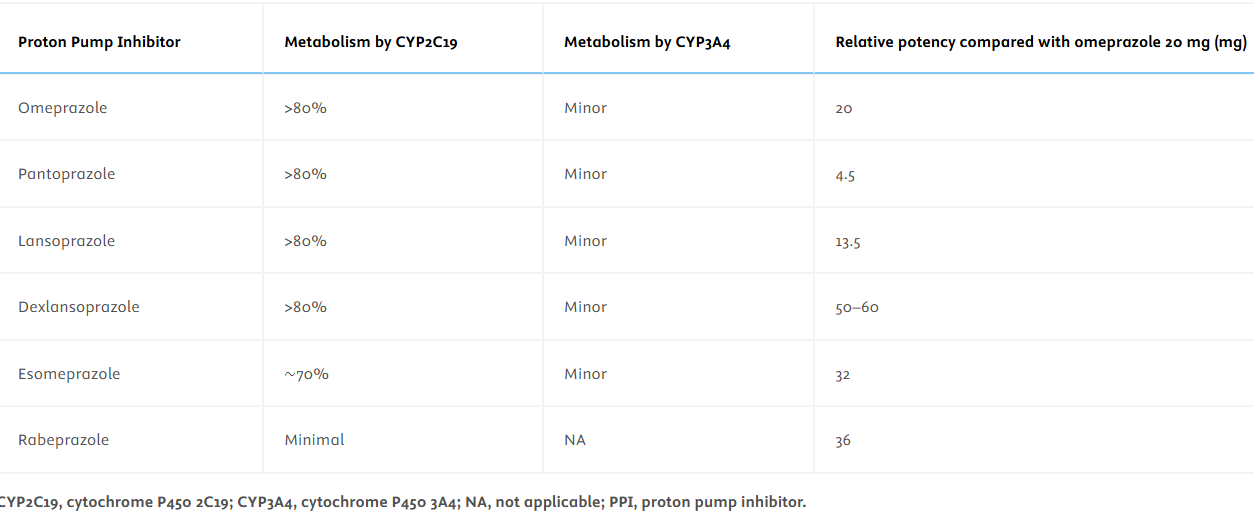
- Among the 184 RMs, 79% (n = 146) had a change in management due to CYP testing results: 65% (n = 120) changed their medication (89 patients were switched to rabeprazole), 22% (n = 41) continued PPI therapy, and 14% (n = 26) increased their PPI dose
Discussion points:
Prevalence of CYP RMs in Other Studies:
- “Ionovo et al studied over 2 million patients who underwent genetic testing using 23andMe and found that the rate of RMs (∗1/∗17) in the general population was 26.0%, and the rate of URMs (∗17/∗17) was 4.4%.25“
- “Fricke-Galindo et al analyzed data from 138 studies of over 52,000 healthy volunteers from around the world.26 The highest rates of combined RMs and URMs were reported in the Middle Eastern populations (36%), followed by European (28.6%), African (16.8%), and Asian populations (3.4%).26 The prevalence was 26.7% in the United States.”
- “Among GI clinical practice guidelines, the 2025 American Society for Gastrointestinal Endoscopy (ASGE) guideline was the first to suggest routine incorporation of CYP testing into the management of patients with GERD.30“
- “PCABs offer a viable alternative to PPIs in patients who are RMs and should be considered accordingly. PCABs are also not dependent on preprandial dosing and thus are easier for patients to take. However, the cost of PCABs continues to be a limiting factor.”
- Testing cost: “A typical out-of-pocket price of $250 to $400 and is covered by some insurance.39“
- Limitations: The study population has a selection bias compared to the general population. Patients referred to a GI clinic are more likely to have treatment-refractory GERD and thus have higher rates of RMs.
My take: In patients with established GERD who are not responding to treatment, CYP testing may be helpful. This is probably true for patients with EoE as well. In patients with GERD who are RMs, options include changing to rabeprazole, higher doses, or possible use of PCABs.
Related blog posts:
- #5000: Simple Rule for Deciding When pH Impedance Testing Should Be Done While on Therapy
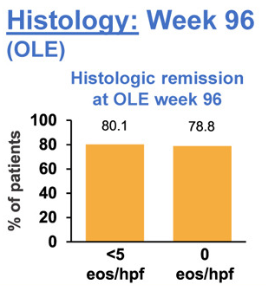
- Updated Data on PPI Effectiveness For Eosinophilic Esophagitis
- How Genetics Influence Response to PPIs in Eosinophilic Esophagitis
- Rome V Pediatric Upper Gastrointestinal Disorders of Gut-Brain Interaction (Part 1)
- Competition for Competitive Acid Blockers
- Incredible Review of GERD, BRUE, Aspiration, and Gastroparesis
- Why Vonoprazan Is More Effective For Erosive Esophagitis Than a Proton Pump Inhibitor
- Gastroesophageal Reflux Phenotypes and “Where Rome, Lyon, and Montreal Meet”
- Why didn’t patient with documented reflux get better with PPI …
- What’s Going On in Patients with Reflux Who Fail to Respond to PPIs?
- How Many Kids with Reflux Actually Have Reflux?