D Ahuja et al. Am J Gastroenterol 2026;121:1192–1201. Comparative Safety of Advanced Therapies in Patients With Ulcerative Colitis: An Administrative Claims-Based Study
Methods: Using an administrative claims database (OptumLabs Data Warehouse) with a ‘real-world’ cohort, the authors identified 9,430 patients with UC treated with TNF antagonists (n = 4,111), anti-integrins (n = 3,165), anti-ILs (n = 1,342), JAK inhibitors (n = 701), or sphingosine-1 phosphate receptor modulators (n = 111), followed over median 27 months.
Key findings:
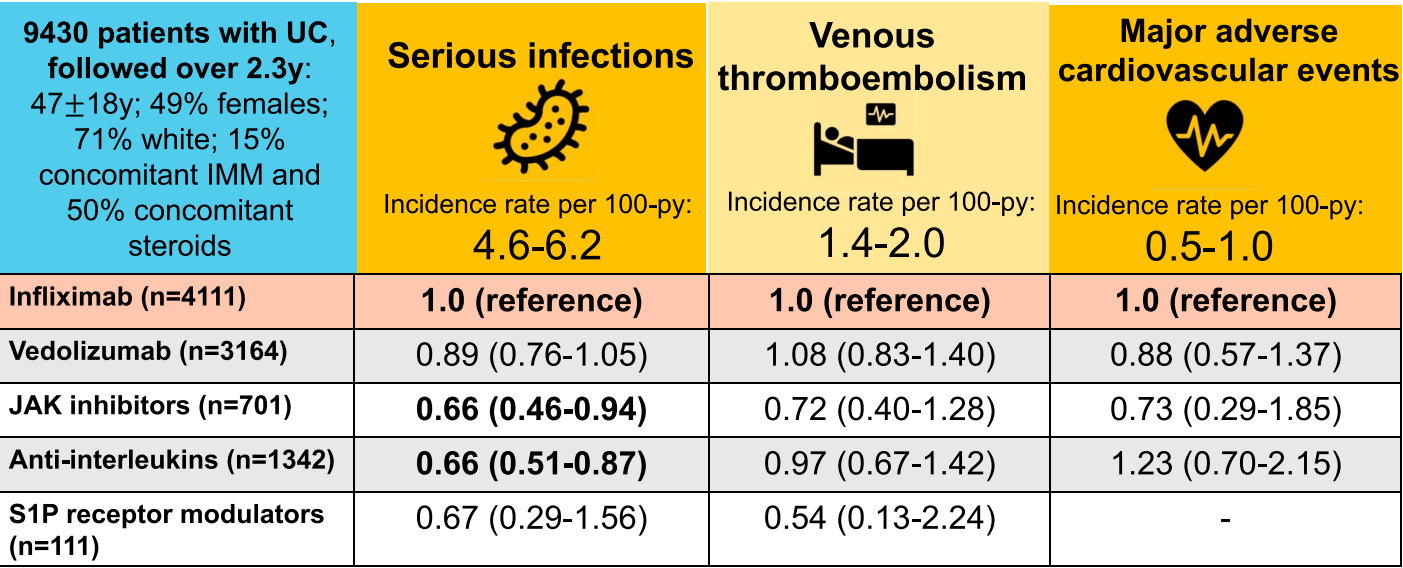
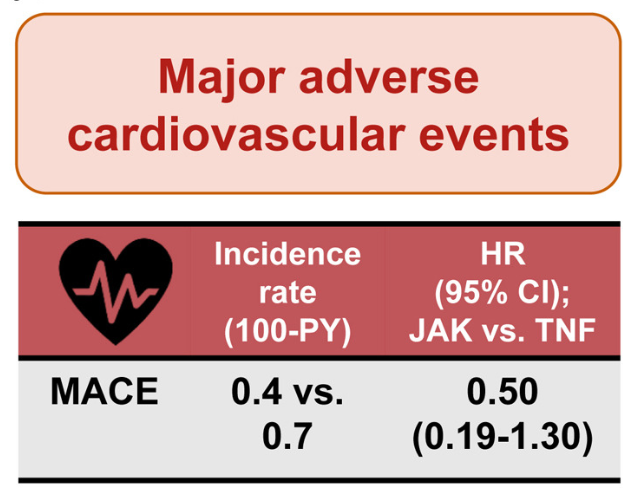
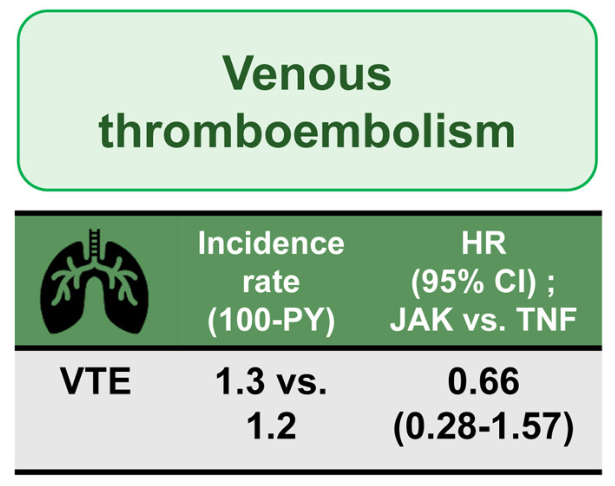
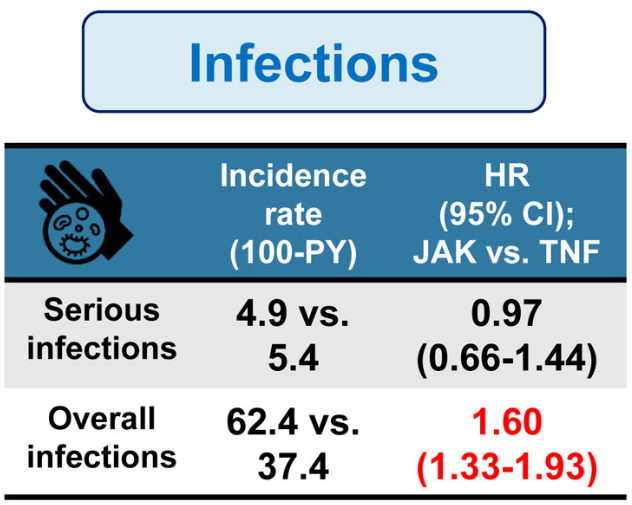
Overall, the risk of serious infections was higher with infliximab than with the other therapies. The incidence of VTE in patients with UC was very low and comparable across all advanced therapies, including JAK inhibitors. Also, the incidence of MACE in patients with UC was
very low and comparable across all advanced therapies, including anti-ILs and JAK inhibitors.
From the discussion: “In a recent network meta-analysis and corresponding clinical guidelines on the management of moderate-to-severe UC, upadacitinib was ranked as having the highest efficacy for induction ofremission compared with all other agents (2,14). However, safety concerns with JAK inhibitors were raised in the pivotal ORAL Surveillance trial (15). In this noninferiority trial, tofacitinib, particularly at higher doses, was associated with a higher risk of serious and opportunistic infections, VTE, and MACE, compared with TNF antagonistsi n patients with rheumatoid arthritis. Following this, the US Food and Drug Administration changed JAK inhibitors’ labeling across all indications, restricting its use in patients with previous failure or intolerance to TNF antagonists…the ORAL Surveillance trial focused on older patients aged 50 years or older with rheumatoid arthritis and at least one cardiovascular risk factor…
[In this study, the] lack of an apparent increase in the risk of JAK inhibitors compared with other medications may be related to superior disease control achieved with JAK inhibitors or reverse causality where patients at high risk of MACE and/or VTE events are not prescribed JAK inhibitors.”
My take: This study provides additional reassurance that newer advanced therapies have similar or better safety than infliximab.
Related blog posts:
- Comparative Safety of Janus Kinase Inhibitors vs Tumor Necrosis Factor Antagonists For Inflammatory Bowel Disease Patients
- Safety of JAK Inhibitors Compared to Anti-TNF Agents
- Comparative Evidence and Positioning Advance Therapies for Inflammatory Bowel Disease
- Prior Exposure to TNF Antagonists May Increase Response to JAK Inhibitors in Patients with Ulcerative Colitis
- FDA Slaps Restrictions on JAK Inhibitors Over Serious Safety Risks
- Dr. Joel Rosh: Positioning Therapies for Pediatric Ulcerative Colitis
- Lipid Changes with IBD Medications