- P Bossuyt et al. Gastroenterol 2026; 171: 99-109. Open Access! The Effect of Dose Intensification After Secondary Loss of Response to Ustekinumab in Crohn’s Disease: Results of the REScUE Study
- J Burisch. Gastroenterol 2026; 171: 24-25 (editorial). Open Access! Reinduction or Redirection? Lessons From the REScUE Trial on Ustekinumab Intensification in Crohn’s Disease
Methods: This was an investigator-initiated, multicenter, randomized, placebo-controlled trial conducted at 15 hospitals in Belgium. Eligible patients were adults (n=108) with CD treated with ustekinumab on maintenance dosing of 90 mg subcutaneous every 8 weeks and experiencing a secondary loss of response. Patients were randomized 1:1 to receiving a single intravenous reinduction with ustekinumab ≈6 mg/kg followed by either subcutaneous ustekinumab 90 mg every 4 weeks or every 8 weeks until week 48.
Key findings:
- Steroid-free clinical remission at week 48 was reached in 15% vs 19% of patients in the every 4 weeks vs the every 8 weeks group
Discussion Points:
- “Remarkably, the overall steroid-free clinical remission rates at week 48 were low in both arms: 15% and 19% for ustekinumab Q4W and Q8W, respectively. Most of the patients achieved clinical remission in the first 24 weeks after IV reinduction though, suggesting that the IV reinduction is the main driver of the effectiveness, rather than the subsequent SC dose intensification.”
- “Our results are in contrast with several retrospective and observational nonrandomized and open-label cohort studies suggesting a clinical response rate after dose intensification up to 60% and clinical remission rates up to 50% after 1 year of treatment.4,13–17“
The associated editorial notes that the modest remission rate could be partly due to a more refractory patient poulation. “The cohort was indeed difficult to treat: median disease duration exceeded a decade, and more than 90% of patients had prior anti–tumor necrosis factor exposure.” Despite this caveat, “the trial avoids overestimating therapeutic success and aligns outcomes with contemporary treat-to-target principles.4 From this perspective, REScUE provides a realistic benchmark for what ustekinumab intensification can and cannot achieve in routine clinical practice.”
The editorial also notes that the “STARDUST trial [which] evaluated a treat-to-target, endoscopy-guided escalation algorithm vs standard of care in ustekinumab-treated CD and did not demonstrate a clear advantage for the intensive, endoscopy-driven strategy at 1 year.7“
My take (borrowed from editorial): “In carefully selected patients who previously responded well to ustekinumab, a short and closely monitored trial of IV reinduction may be considered. However, the threshold for switching to another advanced therapy should remain low if treatment targets are not achieved.”
Related blog posts:
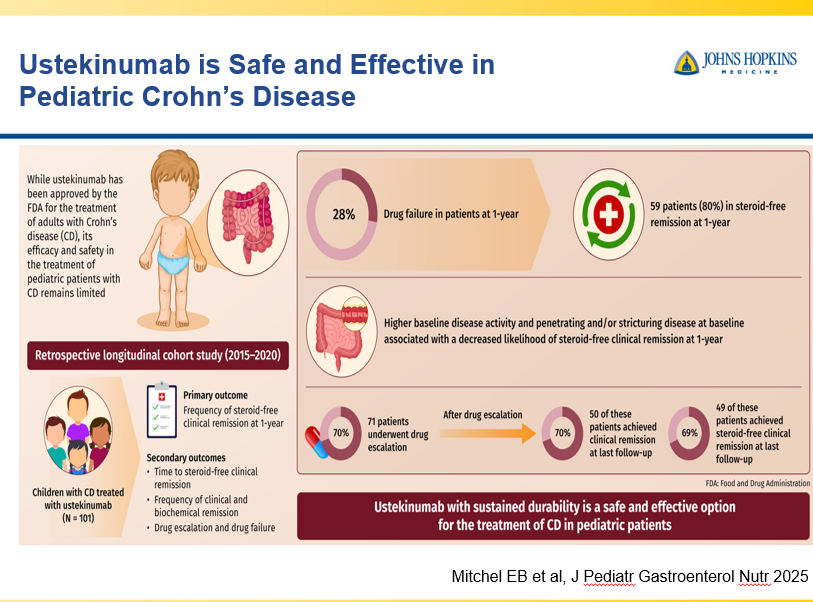
- Real-life Study of Ustekinumab for Pediatric Crohn’s Disease (REALITI Study)
- Ustekinumab Data at 4 Years -UNIFI Extension Study
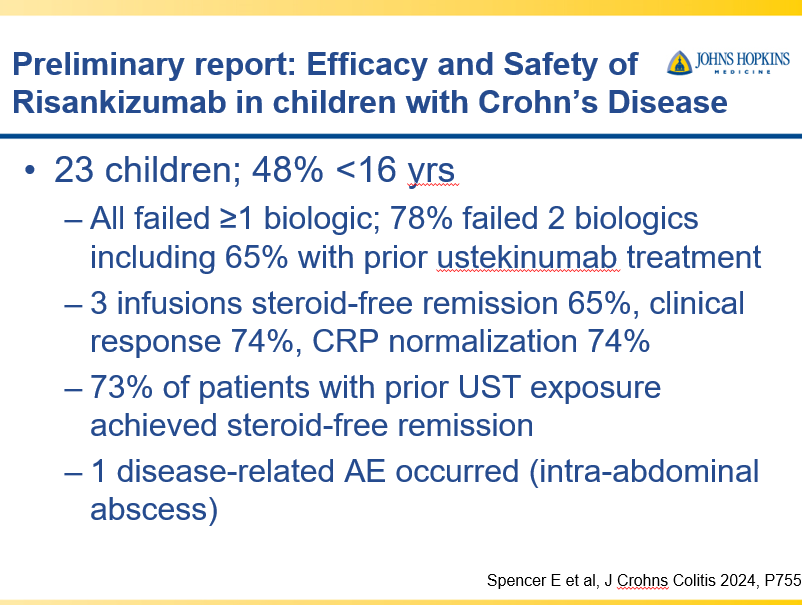
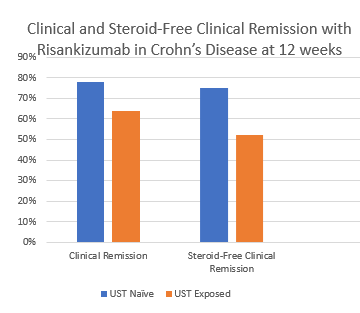
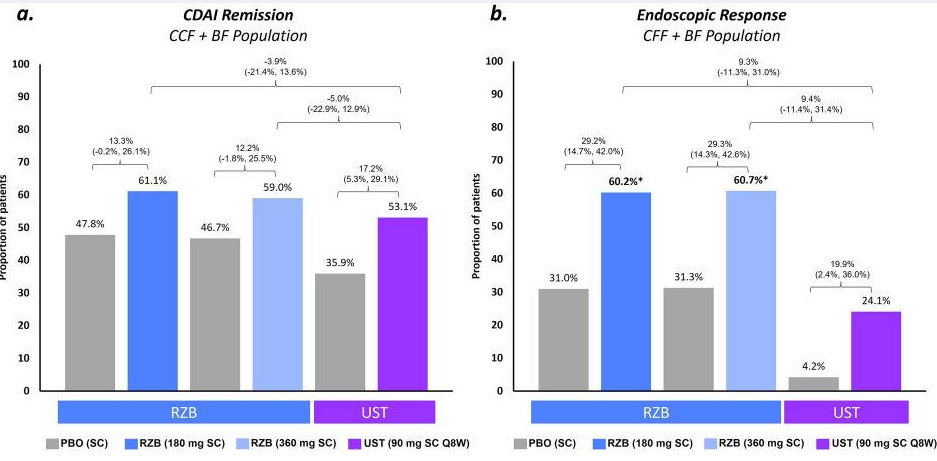
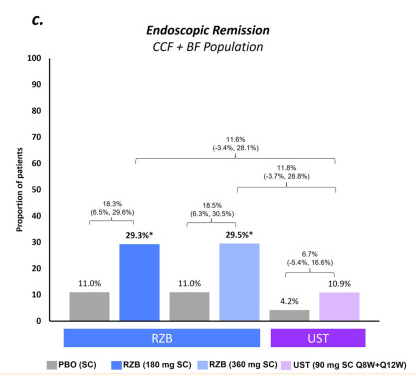
- Risankizumab Outperforms Ustekinumab
- Position Paper: Expediting Drug Approval for Pediatric IBD Ustekinumab approved for pediatric patients 2 yrs and older with Crohn’s disease.