E Louis et al. Clin Gastroenterol Hepatol 2026; 24: 1654-1665. Open Access! Long-Term Safety of Vedolizumab in Patients With Ulcerative Colitis/Crohn’s Disease: A Prospective Observational Study
Methods: This was a prospective, observational, multicenter cohort study in adult patients (n=5208) with UC or CD starting treatment with vedolizumab or other biologics. The primary safety outcome was serious infections compared between cohorts using a Cox proportional hazards model adjusted by propensity score. Clinical effectiveness was a secondary outcome. Mean follow-up duration was 37.4 months. The vedolizumab group had greater age, duration of disease, and concomitant medication use at baseline, indicating more advanced disease.
Key findings:
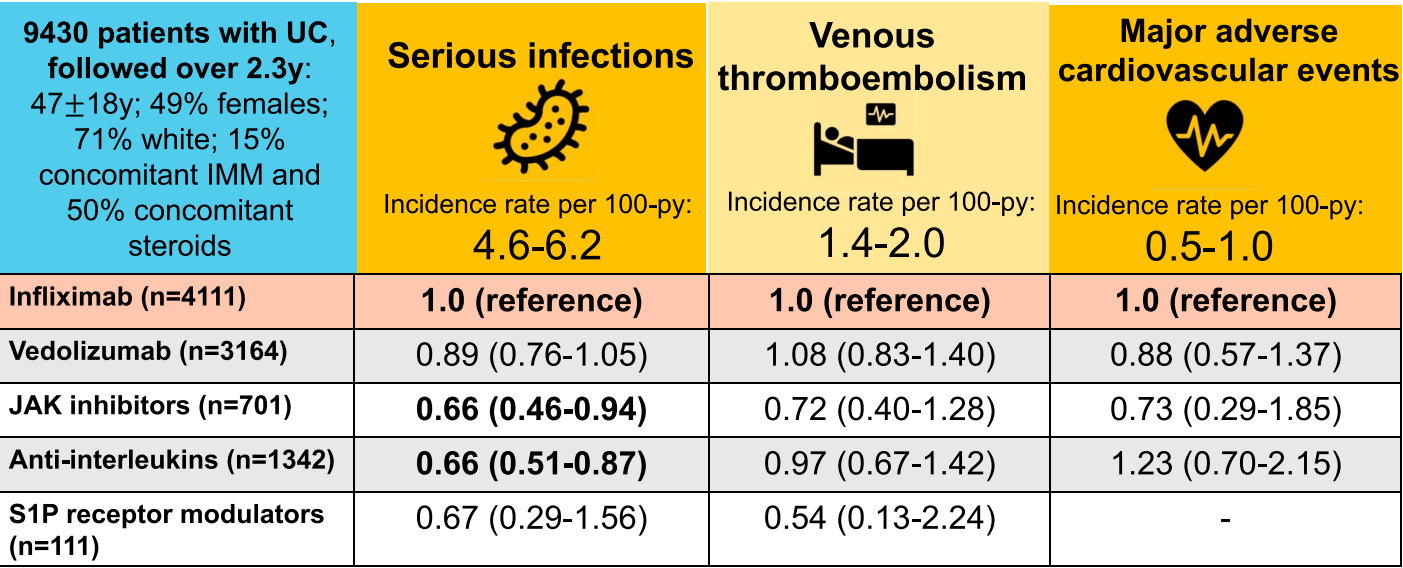
- In patients with UC, the incidence rate per 100 person-years of serious infections was 5.5 (vedolizumab) and 7.0 (other biologic), with an adjusted hazard ratio of 0.89 (P = .38).
- In patients with CD, corresponding findings were 7.9 (vedolizumab) and 6.5 (other biologic) with adjusted hazard ratio of 1.15 (P = .16).
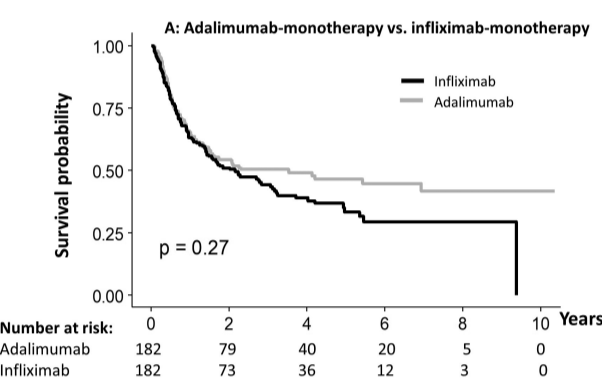
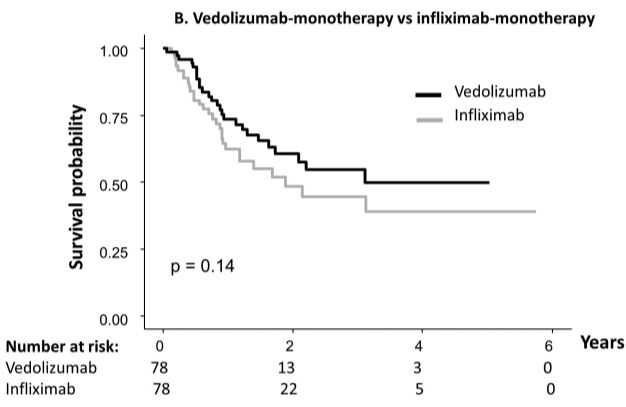
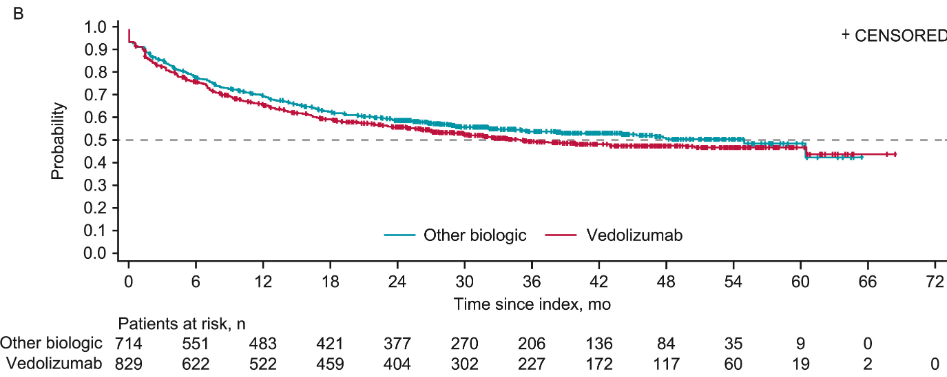
- Rates of clinical response and clinical remission were similar in patients treated with vedolizumab compared with other biologics for both UC and CD.
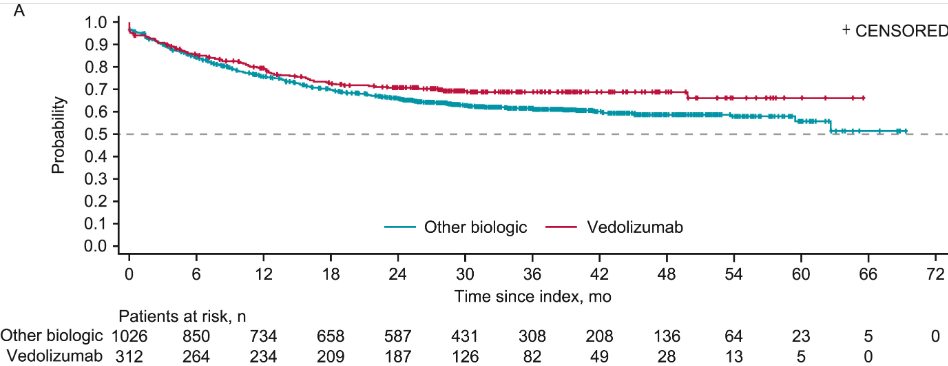
My take: This large prospective study showed no new safety signals with mean followup of more than 3 years. There were no new trends or changes of clinical importance for infections (serious and opportunistic infections, gastrointestinal infections, respiratory tract infections, other infections), malignancies, infusion-related reactions, hepatotoxicity, and pregnancies. No cases of PML were reported. Efficacy was similar between vedolizumab and other biologics.
Related blog posts:
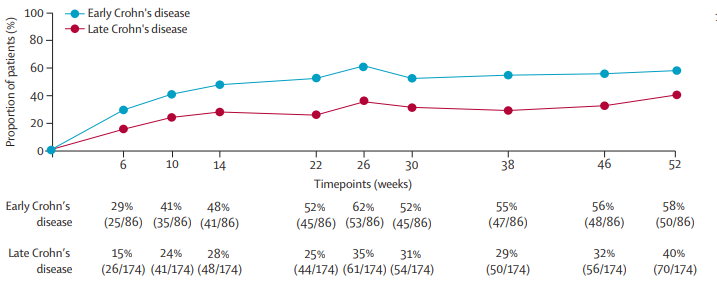
- Comparing Vedolizumab in “Early” and “Late” Crohn’s Disease
- Prior Exposure to TNF Antagonists May Increase Response to JAK Inhibitors in Patients with Ulcerative Colitis (& lower response to vedolizumab) (2025)
- Should Vedolizumab Be Used as a First Line Agent for Crohn’s Disease?
- Vedolizumab’s Impact on Postoperative Crohn’s Disease Recurrence
- Dr. Maria Oliva-Hemker: Positioning Therapies for Pediatric Crohn’s Disease
- What is Mild Crohn’s Disease and How to Treat It
- Comparative Efficacy of Biologics for Crohn’s Disease
- Effects of Thiopurine Withdrawal in Randomized Trial of Vedolizumab-Treated Patients with Ulcerative Colitis
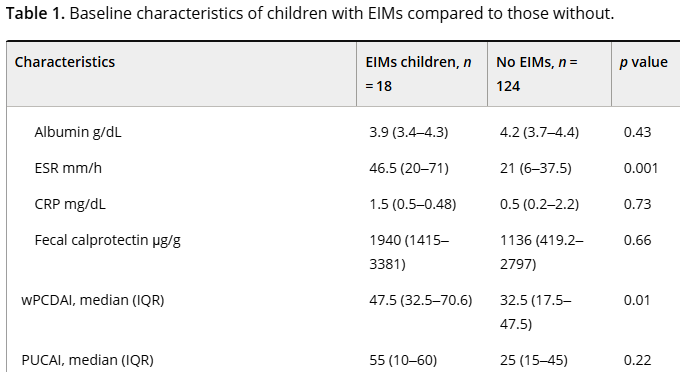
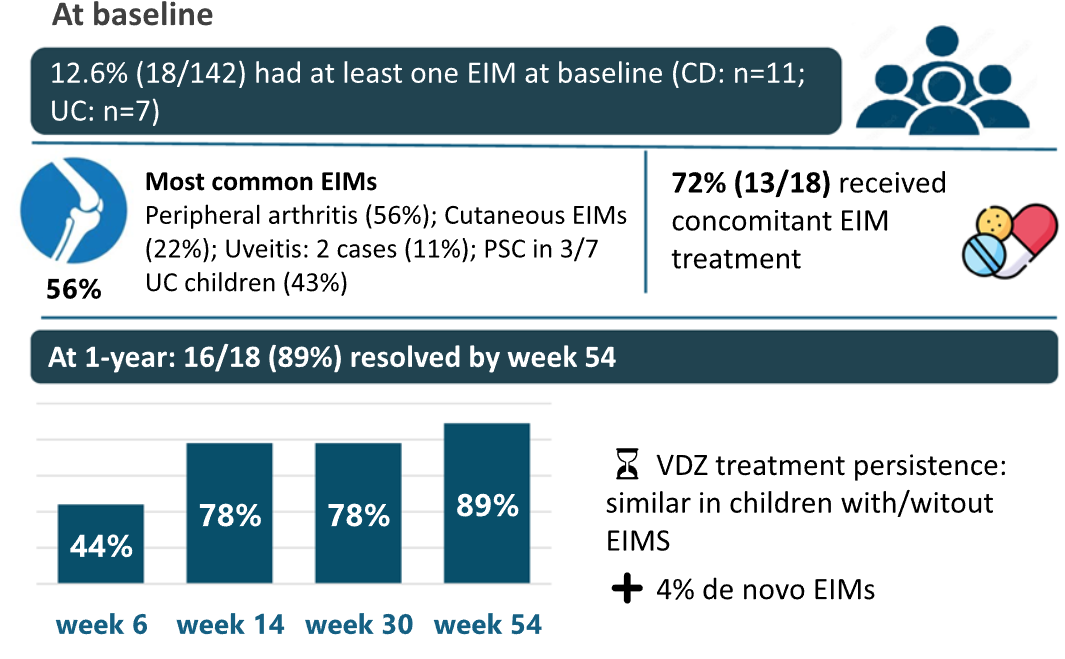
- VedoKids Study: Vedolizumab for Extraintestinal Manifestations of Inflammatory Bowel Disease
- Comparing Infliximab, Adalimumab, and Vedolizumab in Adults and Children with Ulcerative Colitis
- The Importance of the EARNEST Trial –Vedolizumab for Chronic Pouchitis