

SA Kahn, A Bousvaros. JPGN 2022; 75: 418-422. Denials, Dilly-dallying, and Despair: Navigating the Insurance Labyrinth to Obtain Medically Necessary Medications for Pediatric Inflammatory Bowel Disease Patients
This is a very useful review article detailing efforts of insurance companies and pharmacy benefit managers to create hurdles to try to limit the utilization of expensive new medications and how physicians can respond on behalf of their patients.
Key points:
- Pharmacy Benefit Managers: “Typically, third-party payers utilize a pharmacy benefit manager (PBM, middleman) to determine whether a drug will be included in their formulary. In the United States, PBMs include Express Scripts, CVS Caremark, or Optum…[these three] control 89% of the market…these companies restrict access to costly medications and generate a profit for themselves.”
- Lack of FDA Pediatric Indication: “In pediatrics, the average lag time from approval in adults is 9 years…At this time, none of the newer [IBD] agents such as certolizumab, golimumab, vedolizumab, tofacitinib, ustekinumab, and ozanimod are FDA approved for children.”
- Dose Optimization: “TDM [therapeutic drug monitoring] and dose optimization often requires higher doses than those approved by the FDA…result in higher costs for the payer.”
- Step Therapy: “A number of insurance companies follow a “step therapy” algorithm, otherwise known as “fail first formularies…cheaper medication is required before use of a more expensive medication.” Two problems with this approach: these policies in essence force clinicians to “prescribe medications they do not feel are appropriate” and “the majority of these policies are inconsistent with IBD treatment guidelines.”
- Biosimilar/Non-medical switches: “We generally try to educate patients about the clinical data, and endorse switching to biosimilars without appealing the denial.”
- Site of care: “The authors oppose insurance mandated home infusions and suggest appeal of “site of care” switches” due to safety concerns (increase ED visits, infusion reactions), lack of communication with home infusion providers (who often lack pediatric expertise), potential for critical labs not being drawn, and reports of increased loss of response with home infusions.
- Peer-to-peer: “The “peer” may not have the appropriate background…Therefore, …it is very important to inform the peer that the discussion will be documented in the medical record. The clinician should ask for the reviewer’s credentials, specialty, and employer (insurance company, pharmacy benefit manager, or third-party review company).”
- Next Steps: beyond appeal letters (templates at NASPGHAN & CCFA) and peer-to-peer discussions, next steps include an internal appeal (patient files a formal grievance with insurance provider) or external appeal (State Insurance Commissioner). In addition, treatment can be started in the hospital if there are delays in approvals. Though, this could result in the hospital ‘eating’ the cost, the hospital has extensive resources to advocate for coverage and can utilize charitable funds if needed.
My personal experience with appeals:
- For appeal letters, besides including important clinical details, I always try to engage a reviewer’s humanity by explaining how important this approval is for the health of this young boy/girl who faces a lifelong serious illness.
- Most peer-to-peer calls go well but tend to be inconvenient. Lately, I have had several “peer-to-peer” calls with pharmacists who are not authorized to approve the treatment and insist that I schedule a 2nd call with another “peer.”
- Filing a complaint with the State Insurance Commissioner can be very helpful in getting a quick response. In Georgia: Consumer Complaints. It is important to keep the family informed about the status of authorization. A few families have been more successful/persistent at navigating this process than those with years of experience.
My take: This is a helpful and timely article. Trying to quickly get medications authorized is needed to avoid delays in patient care that could result in harm.
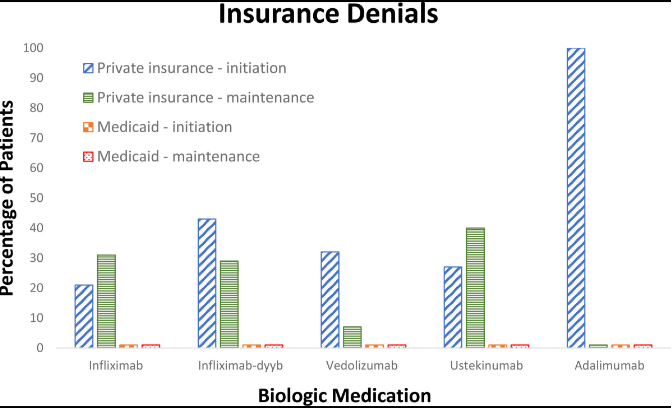
Related article: CA Lepus, JS Hyams. JPGN Reports. 2022; doi: 10.1097/PG9.0000000000000215. Open Access! Barriers From Third-Party Payers to Biologic Use in Pediatric Inflammatory Bowel Disease This study prospectively identified pediatric patients with IBD who were started on a biologic medication at our institution, and third-party payer decisions were recorded:
- “The average time between TPI (therapy plan initiation) and biologic initiation (first infusion) was 9.7 days (±3.7 days) for patients with Medicaid, 11.3 days (±5.2 days) for patients with private insurance who had approvals, and 18.8 days (±7.6 days) for patients with private insurance who initially had denials”
- “Reasons for denial are generally for use of a specific off-label agent or dosing of an approved agent. These denials lead to delayed treatment, nonmedically sound changes in therapy, and increased administrative burden on providers.”
- “Despite the growing body of literature supporting use of [proactive] TDM (therapeutic drug monitoring), third-party private payers customarily deny adjustments unless the patient is symptomatic, a situation that clinicians try to avoid.”
Related blog posts:
- The Consequences of Prior Authorizations
- FDA IBD Workshop -Take-Home Points Off-label does not equate to experimental FDA Statement: The FD&C Act does not, however, limit the manner in which a physician may use an approved drug. Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling. Such “unapproved” or, more precisely, “unlabeled” uses may be appropriate and rational in certain circumstances, and may, in fact, reflect approaches to drug therapy that have been extensively reported in medical literature
- “We Need More Information to Process This Claim” | gutsandgrowth
- More on High Drug Costs (Humor)
- For the Next Insurance Appeal: Therapeutic Drug Monitoring in Adalimumab Treatment (Pediatrics) & Satire on Prior Authorizations
- Expert Consensus: New Recommendations for Therapeutic Drug Monitoring | gutsandgrowth

Have had recent personal experience with a pharmacist at CVS caremark who agreed with my clinical argument, but was not authorized to approve the physician’s appeal. Was told there was no higher point of escalation (pulmonologist had already submitted PA and appeal) and I needed to pay 300 dollars a month cash for the prescription (asthma controller).
I am doing so, but can imagine many families in my spot who would not be able to.
Is it hyperbolic to say that PBMs have blood on their hands?