G D’Arcangelo et al. J Pediatr Gastroenterol Nutr 2026; 83: 96-107. Open Access! Impact of 5-Aminosalicylic acid discontinuation in children with ulcerative colitis on biologic therapy: A propensity score-matched study
Background: Several adult-based studies have found that discontinuing 5-ASA at the initiation of anti-TNF therapy is not associated with worse clinical outcomes. “Ungaro et al. analyzed data from over 3500 patients in the United States and Denmark and found no increased risk of adverse outcomes following mesalamine discontinuation after the initiation of anti-TNF therapy.18 Based on this evidence, the American Gastroenterological Association recommends discontinuing mesalamine in patients with moderate-to-severe UC who are starting biologics or small molecules and achieve remission.19 However, this recommendation is based on low-quality evidence, and pediatric guidelines do not offer a similar directive.2“
Methods: Retrospective, multicenter, case–control study which included 227 pediatric patients in the final analysis after matching (85 [37.5%] cases and 142 [62.5%] controls].
Key findings:
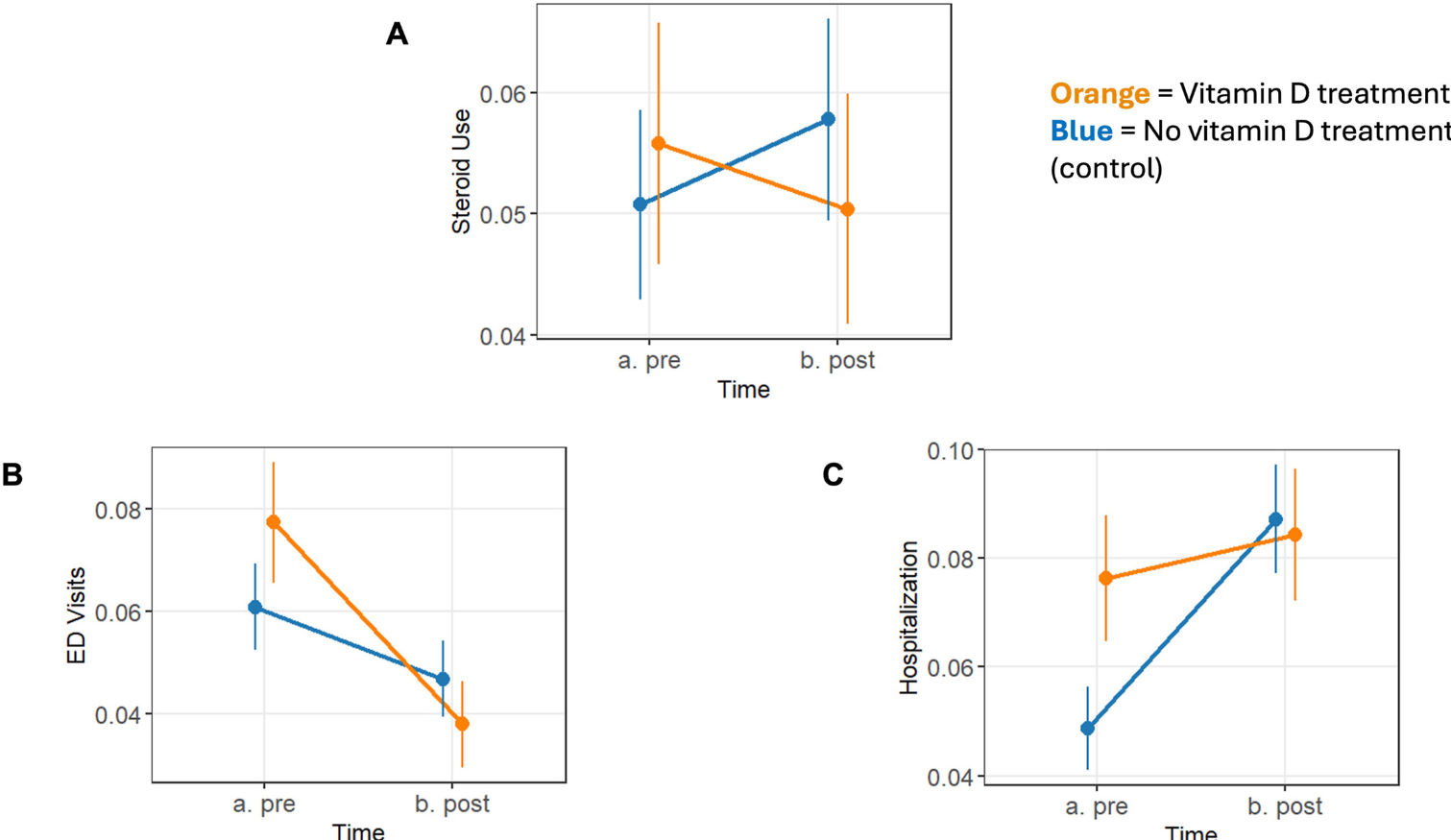
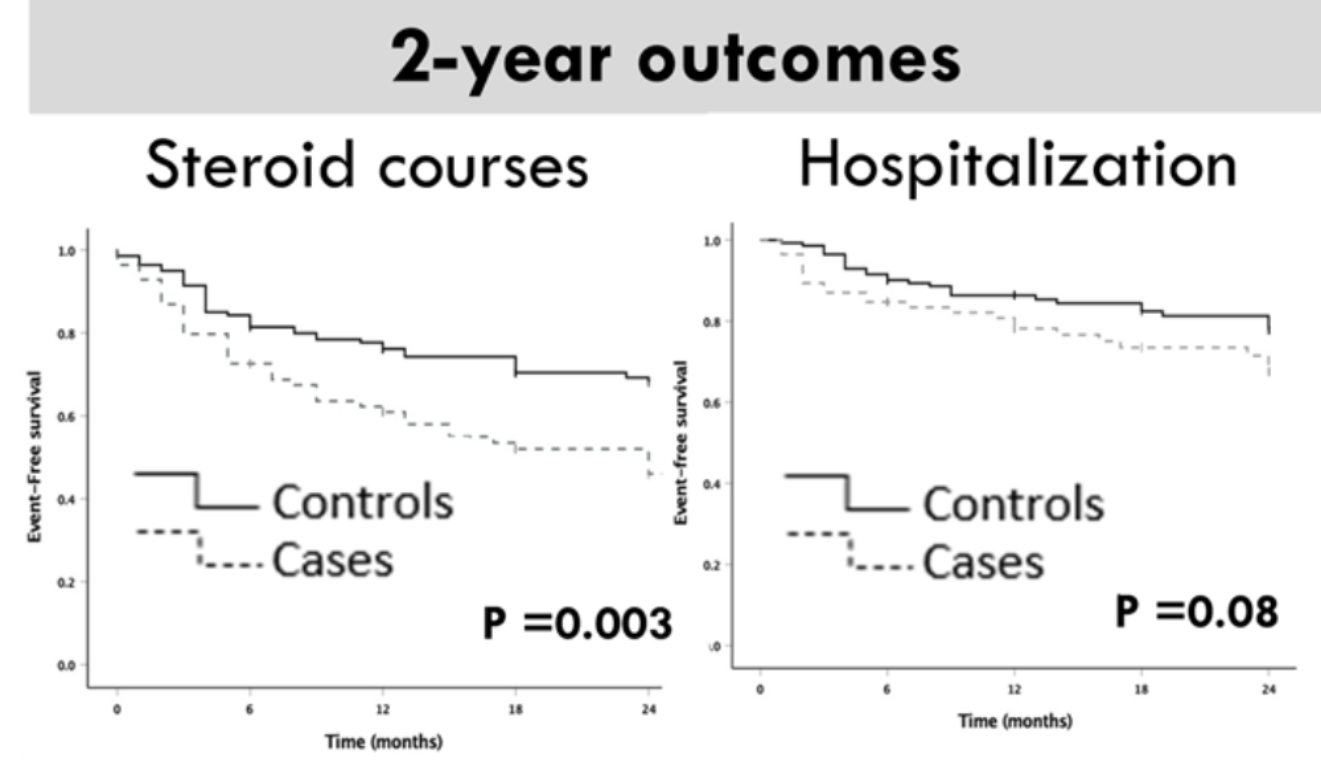
- Children who discontinued 5-ASA were at higher risk of courses of steroids (Log-Rank p = 0.003) and hospitalization (p = 0.08). This finding persisted with multivariate Cox regression analysis.
- “Fixed timepoint analyses showed a statistically significant increase in the odds of adverse outcomes at the 6-month follow-up (including hospitalizations and acute severe colitis), with no significant differences detected at 12, 18, or 24 months, and only a non-significant trend toward higher hospitalization risk over time.”
My take: This is an intriguing study with a small sample size of pediatric IBD patients. Given the findings in adults, it is customary to stop 5-ASA at the time of initiation of biologic therapy. However, this study indicates that pediatric patients—who often present with more extensive and severe disease—may have some benefit from overlapping these therapies, especially during the first six months. A prospective pediatric study would be helpful.
Related blog posts:
- Sulfasalazine vs 5-ASA: Treatment Outcomes in Pediatric UC
- “For Hospitalized Patients With ASUC, 5-ASA Adds No Value to Steroids”
- Images Only: Combined 5-ASA/Biologics in Ulcerative Colitis, & Carbohydrate Intake and Health
- Pediatric Guidelines for Ulcerative Colitis (Part 2: Acute Severe Colitis)
- AGA Guidelines: Moderate to Severe Ulcerative Colitis
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition