
R Rosen et al. Gastroenterol 2026; 170: 1347-1366. Open Access! Rome V Pediatric Upper Gastrointestinal Disorders of Gut-Brain Interaction
This article has a lot of useful information and I recommend reading the article in full. The disorders covered include the following:
Esophageal Disorders:
- Reflux hypersensitivity
- Reflux-negative esophageal pain disorder (similar to functional heartburn in adults)
- Aerophagia syndrome
- Supragastric belching syndrome
Functional Pediatric Feeding Disorders
- Hypersensitvie dysphagia
- Anticipatory Restrictive Feeding
- Hunger dysregulation feeding disorder
- Medically-triggered functional feeding disorder
Gastroduodenal Disorders
- Rumination Syndrome
- Cyclic Vomiting Syndrome
- Cannabinoid hyperemesis subgroup
- Chronic Nausea
- Functional Dyspepsia
- Postprandial Distress Syndrome
- Epigastric Pain syndrome
The authors note that the Rome V criteria have expanded to include several more disorders. “This expansion provides a diagnostic framework for patients presenting with chest and throat pain, feeding difficulties, belching, pain with eating, nausea, and vomiting. Given the advances in impedance technology and high-resolution manometry, testing plays a greater role in many of these diagnostic criteria than they have in past Rome iterations. This harmony between symptoms and testing results in more precision in therapeutic approaches that are critically multidisciplinary. The ability to assign new, positive diagnoses across the upper gastrointestinal tract offers new opportunities for pediatric-focused therapeutic trials.”
With regard to esophageal disorders, the key points:
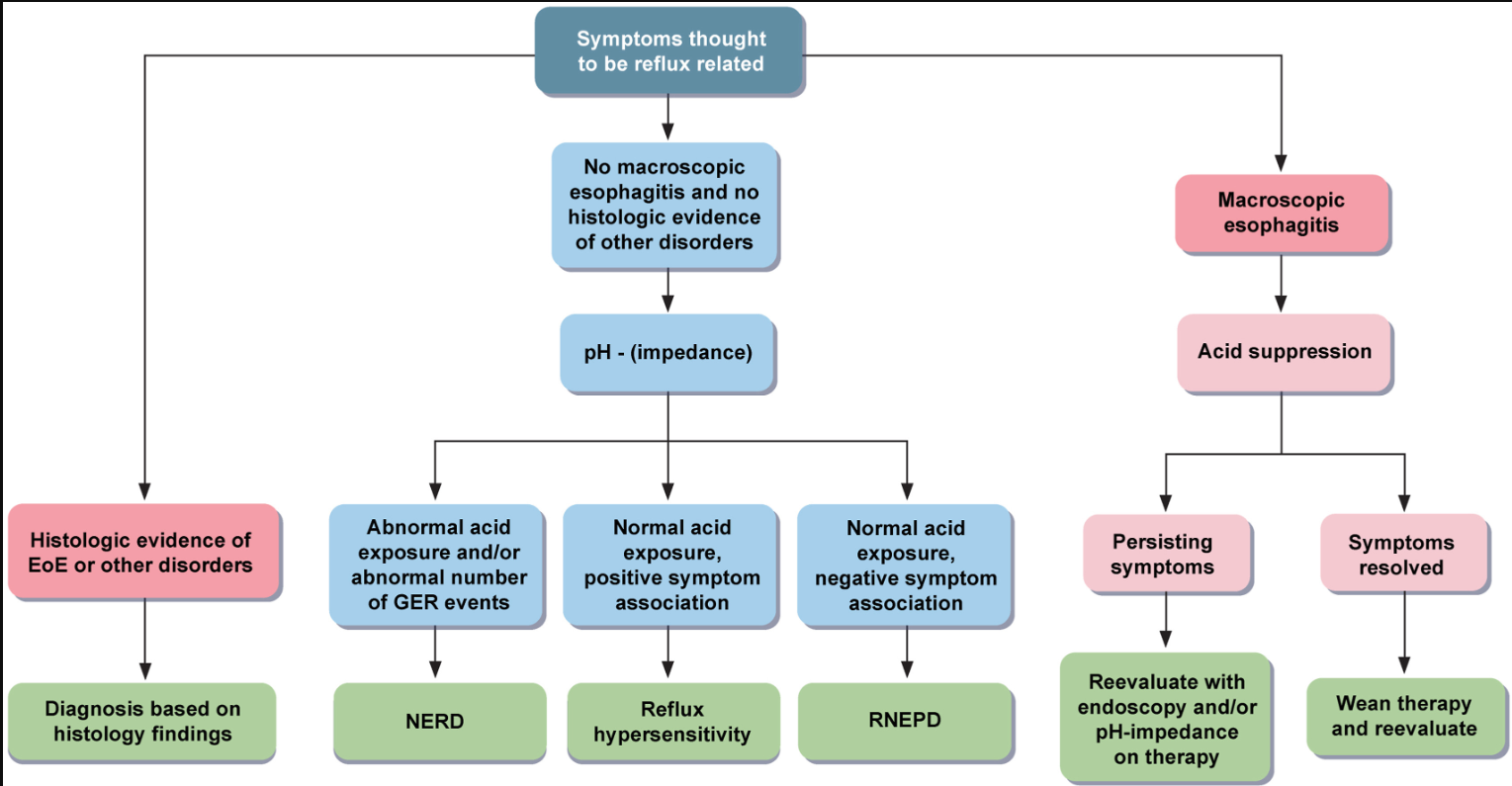
- “In the past, nonerosive reflux disease was the all-encompassing diagnosis for children without pathologic amounts of gastroesophageal reflux. The use of pH-impedance testing has allowed for additional phenotyping of patients with significant symptoms that are typically associated with gastroesophageal reflux disease”
- “PPI response does not reliably predict reflux phenotype…Empiric acid suppression trials should be time-limited up to 8 weeks and further diagnostic testing (ie, endoscopy, pH-impedance, and CYP2C19 gene testing if possible) should be pursued if there is no symptom improvement.20 Histamine-2 receptor antagonists can also treat esophageal hypersensitivity and are a first-line therapy for patients awaiting endoscopy.”
- “Patients with reflux-negative esophageal pain disorder (RNEPD) have a visually normal upper endoscopy and no evidence of pathologic acid reflux with negative reflux-symptom correlation by pH-impedance (or pH-metry or wireless testing). This is equivalent to functional heartburn (FH) in adults. However, unlike adult FH, symptoms of RNEPD may include intermittent retrosternal pain, heartburn, throat pain, or burning sensation in the throat, at least 3 times per week for 2 months.31 Younger children may present with crying or repeatedly pointing to areas of discomfort. Two studies found that 38%–44% of pediatric patients with normal endoscopy undergoing pH-impedance testing met criteria for FH per the adult Rome IV definition.3,4…Because RNEPD falls on the spectrum of visceral hypersensitivity, neuromodulators should be the mainstay of therapy”
- “Aerophagia, a normal physiologic phenomenon, should only be considered a syndrome if it impacts quality of life and causes symptoms. Previously, increased flatus was considered a major criterion but because flatus may go unnoticed, it is no longer a major criterion…Treatment No therapeutic trials exist. However, in patients with severe distention, a nasogastric tube or an existing gastrostomy tube can be used to vent air from the stomach.55 If colonic distention is present, rectal decompression may be appropriate. In patients with chronic stable symptoms, a conservative approach is sufficient. Speech therapy or CBT aimed at reducing the air swallowing may be tried. Benzodiazepines can be considered in severe cases. Circumstantial evidence suggests that infants swallow less air using different bottle or nipple systems.56“
- Supragastric Belching Syndrome “SGB is a voluntary yet subconscious behavior…Most patients present with excessive belching as the primary symptom. However, the symptoms may sound like hiccups to patients or parents. Often no tests are needed, as the story of multiple repeated belches is nearly pathognomonic for SGB. SGB typically occurs outside of meal periods and does not occur during sleep. pH-impedance or HRIM can be performed to confirm the diagnosis. However, absence of belching during testing does not exclude the diagnosis, as events can be sporadic. Treatment In a single randomized trial of behavioral interventions in adults, which included education about the disorder, warning signs for oncoming events, and breathing exercises, patients who received the behavioral interventions had higher rates of symptom improvement lasting up to 6 months”
Related blog posts:
- Differentiating NERD from Functional Heartburn
- What’s Going on With Refractory Heartburn?
- Jose Garza: Belching, Bloating and Best Advice
- Expert Advice on Bloating, Belching and Distention
- Dr. Neha Santucci: Management of DGBIs in the Post-Pandemic Era (Part 1)
- Understanding Hiccups Plus TikTok & Unhealthy Eating Habits
