AS Mayer,et al. Arthritis Care Res. https://doi.org/10.1002/acr.80067. Open Access! Safety of Prescription Nonsteroidal Anti-inflammatory Drugs in Adults With Inflammatory Bowel Disease: Data From a Large Administrative Claims Cohort.
Methods:
- “This retrospective cohort study included patients with IBD aged at least 18 years from Optum’s deidentified Clinformatics Data Mart Database (2000–2022). Patients with a new NSAID prescription fill were matched to those without an NSAID fill during the study period…Propensity score-based inverse probability of treatment-weighted Cox proportional hazards models evaluated the association between NSAID exposure and time to IBD-related hospitalization across IBD subtypes.”

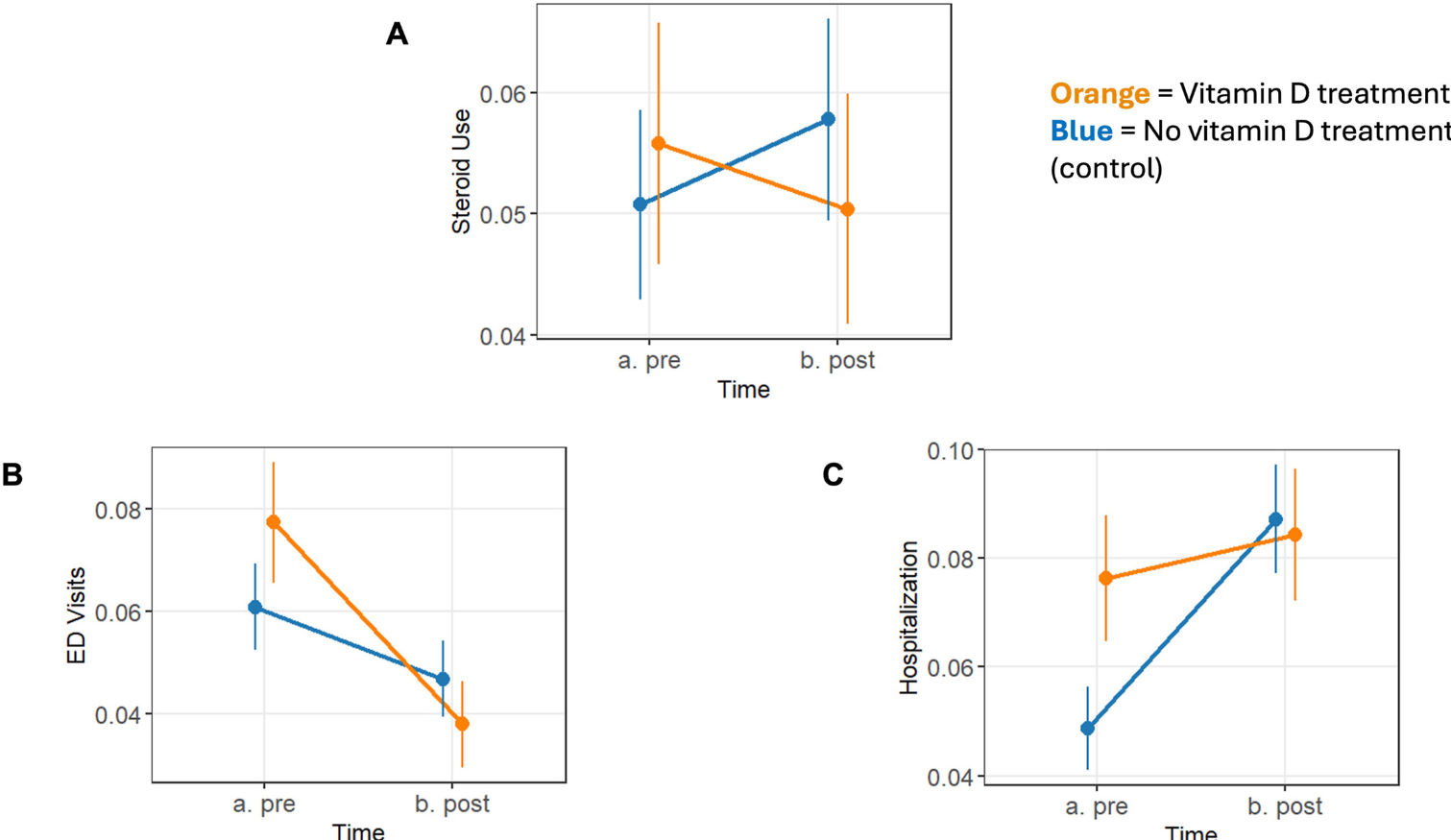
Key findings:


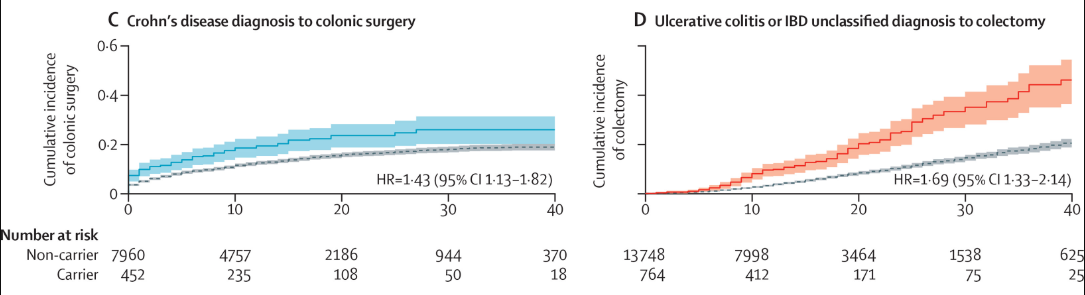
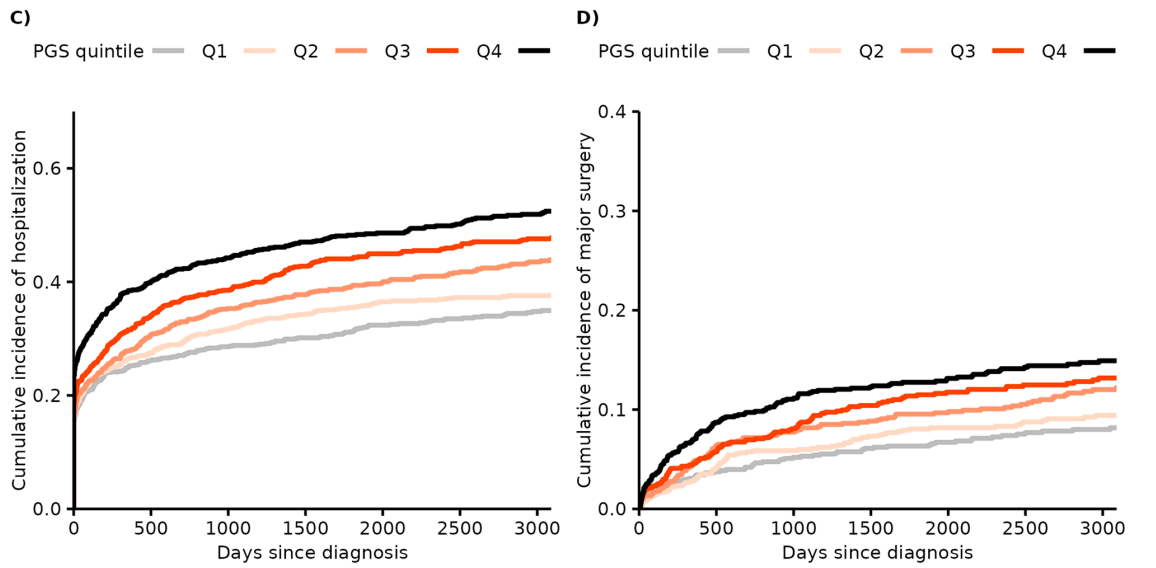
with Crohn disease (B).

with ulcerative colitis (C).
Discussion:
- “The use of IPTW [inverse probability of treatment weighting] to balance an extensive number of confounders associated with NSAID use optimizes the assessment of the association of NSAID exposure with IBD-related hospitalization and helps address recent concern of residual confounding in observational studies of NSAID risk in IBD.”
- Besides the potential risk of an IBD flare, “NSAID use is associated with risk of hospitalization from several non-IBD–related entities such as acute kidney injury and adverse cardiac events…a large prospective multicenter observational study of more than 18,000 admitted patients in England found that NSAIDs were responsible for 29.6% of admissions related to adverse drug reactions, including gastrointestinal bleeding, stroke, and renal impairment.34“
My take: This study shows an association of increased hospitalization in patients with CD but not UC based on NSAID exposure. The absolute risk of this appears low and could be in fact related to residual confounders (despite use of IPTW) as this was not a prospective study. The risk of NSAIDs outside the GI tract are likely more significant for most patients. Nevertheless, there are limited options for pain management and NSAID benefits have to be weighed against other approaches.
Related blog post: Rethinking the Link between NSAIDs and IBD Flares