N Gonsalves, E Dellon E, K Kliewer K et al. The Lancet Gastroenterology & Hepatology, 2026; DOI: 10.1016/S2468-1253(26)00116-0. Open Access! Dupilumab versus placebo in adults and adolescents with eosinophilic gastritis (DEGAS): a double-blind, placebo-controlled, phase 2, multicentre, randomised controlled trial
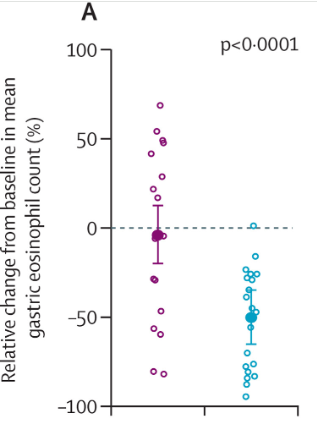
Methods: This was a phase 2b trial with a 12-week, double-blind, placebo-controlled period, followed by a 24-week open-label extension period. Patients aged 12–70 years from 11 hospitals in the USA with histologically active eosinophilic gastritis (≥30 eosinophils per high-power field [HPF] in at least five HPFs in the gastric antrum and/or body) and moderate-to-severe symptoms. Eligible patients were individually randomised (1:1) to parallel groups and received six injections over 12 weeks: subcutaneous dupilumab (n=21) (600 mg once followed by 300 mg every 2 weeks) or subcutaneous placebo (n=20). The primary endpoint of relative change from baseline in mean gastric eosinophil count.
Key findings:
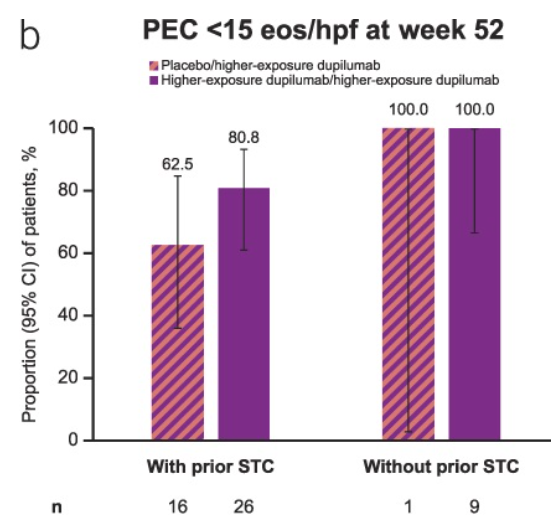
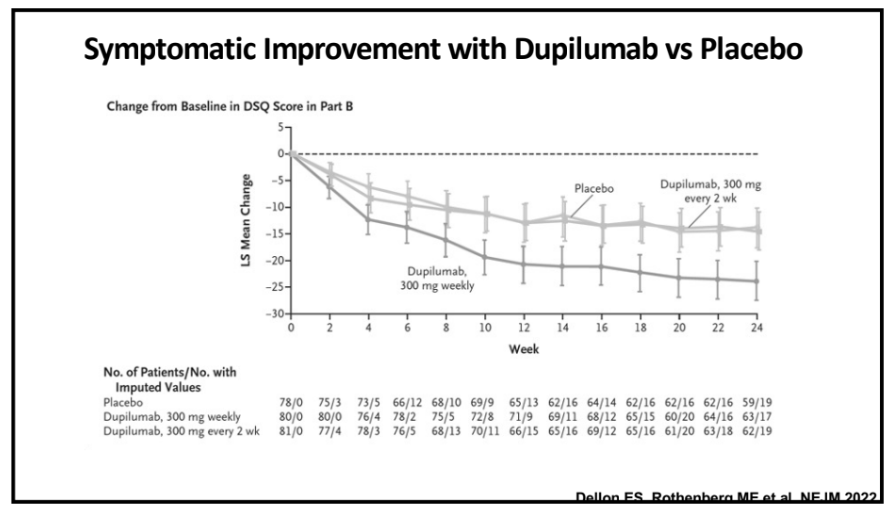
- At week 12, the relative reduction in the primary endpoint was greater with dupilumab (estimated mean change –50%) than with placebo (–4%)
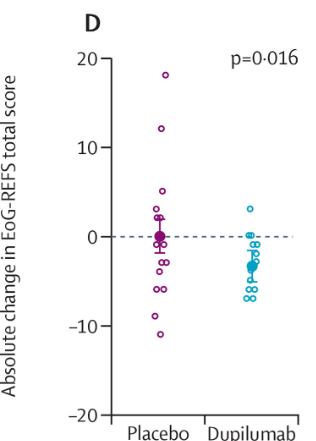
- Reduction from baseline in EoG-REFS (Eosinophilic Gastritis Endoscopic Reference Score) at week 12 was greater with dupilumab (estimated mean change –3·47 points than with placebo (–0·06 points)
Discussion Points:
“Currently, there are no FDA-approved therapies for patients with eosinophilic gastritis…this first prospective trial of dupilumab for eosinophilic gastritis show a greater reduction in mean gastric eosinophil count from the five most eosinophil-dense HPFs (the primary endpoint) with dupilumab compared with placebo.”
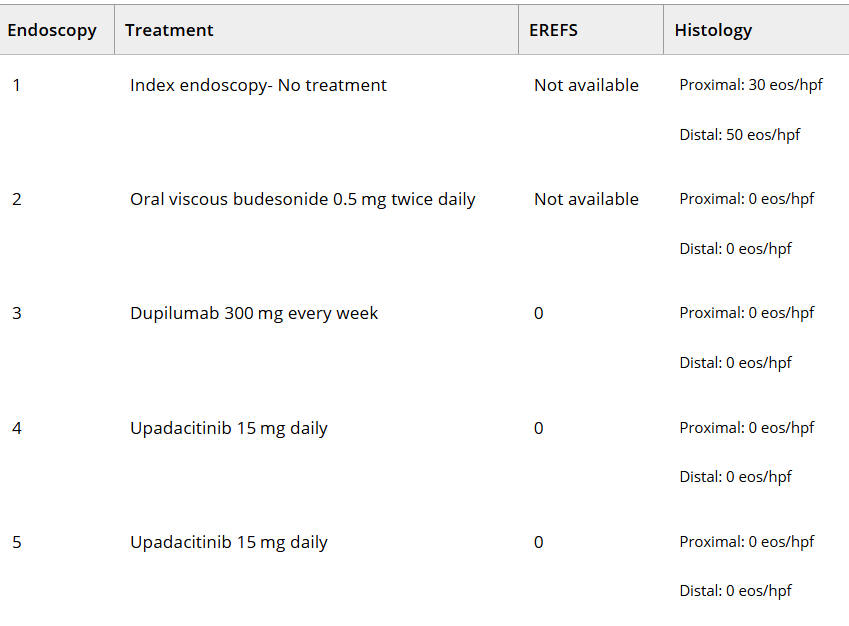
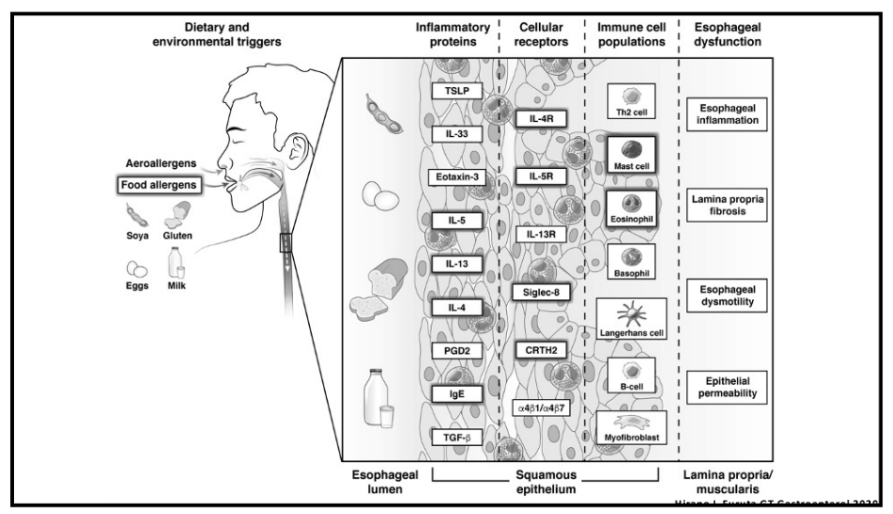
My take: Dupilumab improved eosinophilic gastritis histology and endoscopic appearance. This study suggests that there may be overlapping pathophysiology between eosinophilic gastritis and eosinophilic esophagits as dupilumab appers to be effective in both disorders.
Related blog posts:
- 2026 Review: Eosinophilic Gastrointestinal Diseases (EGIDs)
- How Closely Related Are Eosinophilic Gastrointestinal Disorders To Isolated Eosinophilic Esophagitis
- Eosinophilic Gastritis -Pathogenesis Is Not Just the Eosinophils or Benralizumab Would Work
- Endoscopic Assessment of Eosinophilic Gastritis
- Updated Nomenclature for Eosinophilic Gastrointestinal Diseases
- Two Studies for Eosinophiles