
N Wolfest et al. Clin Gastroenterol Hepatol 2026; 24: 1271-1279. Open Access! Efficacy of Dupilumab on Facilitated Food Reintroduction in Eosinophilic Esophagitis
Methods: This open-label pilot study — patients who demonstrated disease control in the dupilumab run-in stage were able to continue into the food reintroduction stage for a total of 52 weeks. Reintroduction of trigger foods occurred at months 3, 6, and 9, while continuing on dupilumab treatment. Symptoms, histology, endoscopy, and esophageal diameter were compared prior to and following every phase of food reintroduction to month 12. All patients had previously failed trigger food reintroduction on their current EoE medication.

Key findings:
Dupilumab effectiveness: At month 3 of the dupilumab run-in stage, 17 of 19 evaluable patients (89%) per protocol had a PEC (peak eosinophil count) of <6 eos/hpf. One patient had a PEC of 6 eos/hpf but was permitted to proceed to the food reintroduction stage.
Food reintroduction:
- Reintroduction of an EoE trigger food was successful in 86% of instances (54/63), as defined by a PEC <6 eos/hpf and no symptoms
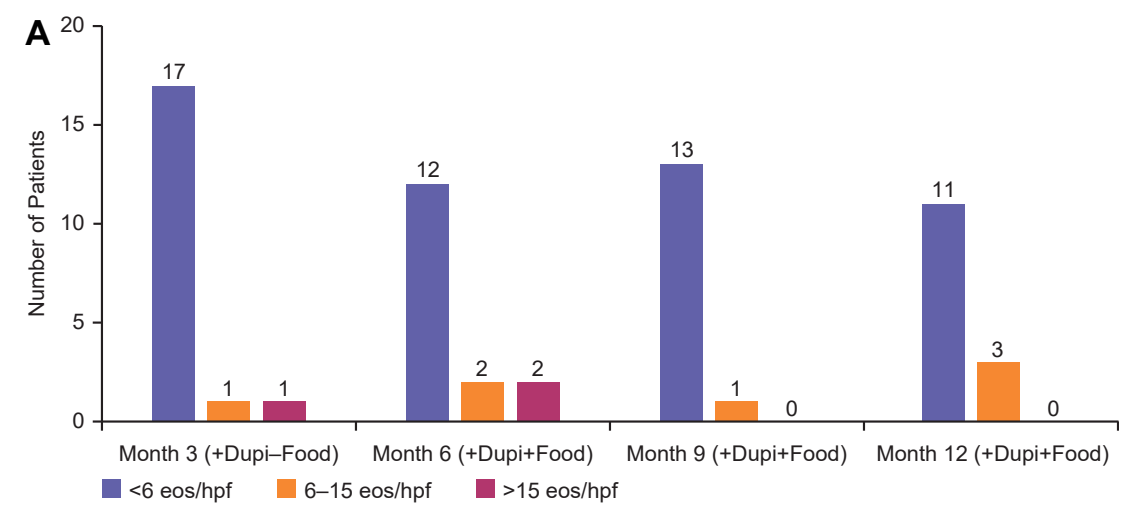
- At month 6, 75% of patients (12/16) successfully reintroduced an EoE trigger food, and, as portion size was increased or additional trigger foods were added, 93% (13/14) and 79% (11/14) successfully introduced EoE trigger foods at months 9 and 12, respectively
- By the end of the study, 5 patients successfully achieved unrestricted serving sizes of an EoE trigger food without worsening esophageal biopsies
- The mean PEC did not significantly change following food reintroduction at month 6 (5.3 [SD, 8.9]), month 9 (1.3 [SD, 2.8]), or month 12 (2.6 [SD, 4.5]) (see Figures below)

My take (borrowed in part from authors): For most newly-diagnosed patients, the majority prefer medical therapy over dietary restricitons. In those currently managed with dietary restrictions, “dupilumab treatment may provide a safe method for patients with EoE to gradually taper elimination diets for some trigger foods.”
Related blog posts:
- ESPGHAN Eosinophilic Esophagitis Guidelines
- “Real-World” Dupilumab for Eosinophilic Esophagitis
- Practical Tips for Eosinophilic Esophagitis
- 1-Food vs 4-Food Elimination Diet for Eosinophilic Esophagitis
- Eosinophilic Esophagitis -Increasing Incidence and Emergence of Biologic Treatments
- Practical Guide to Dietary Therapy for Eosinophilic Esophagitis
- Dupilumab (Dupixent) for Young Children with Eosinophilic Esophagitis (Published Data)
- Dupixent Approved in Younger Children (15 kg+)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
