M Chehade et al. Am J Gastroenterol 2026; 121: 649-660. Open Access! Dupilumab Efficacy in Children With Eosinophilic Esophagitis With Prior Swallowed Topical Corticosteroid Use: A Subgroup Analysis Thanks to Ben Gold for this reference.
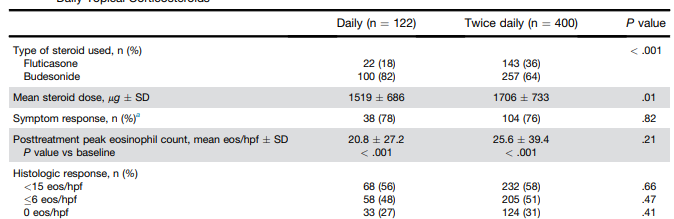
Background: “The aim of this exploratory, post hoc subgroup analysis of EoE KIDS was to assess dupilumab efficacy and safety in patients aged 1–11 years with EoE previously treated with STCs” [swallowed topical corticosteroids]. This study further examined th EoE KIDS cohort (Chehade M, Dellon ES, Spergel JM, et al. Dupilumab for eosinophilic esophagitis in patients 1 to 11 years of age. N Engl J Med 2024;390(24):2239–51.)
Methods: The trial consisted of the following: part A, a 16-week, randomized, double-blind, placebo-controlled treatment period; part B, a 36-week, extended active treatment period in which patients knew that they received active treatment but did not know their regimen; and part C, a 108-week, open-label extension period in which all patients received higher-exposure dupilumab. Eligible patients were aged 1–11 years with a confirmed diagnosis of active EoE who were unresponsive to ≥8 weeks of PPIs.
Of 102 patients, 82 (80%) received prior STCs and 59 (58%) had prior inadequate response, intolerance, and/or contraindication (IRIC) to STCs.
Key findings:
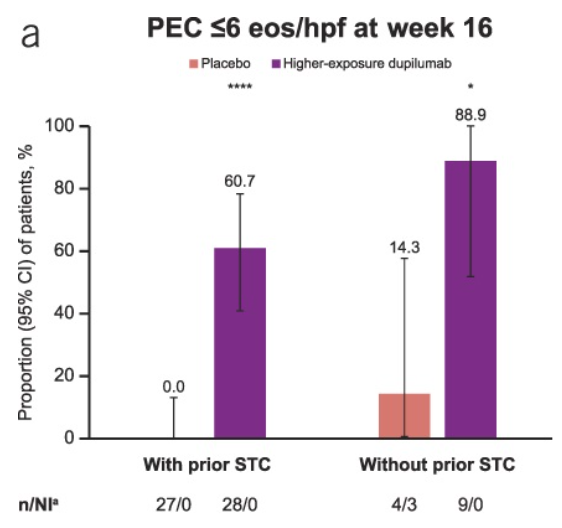
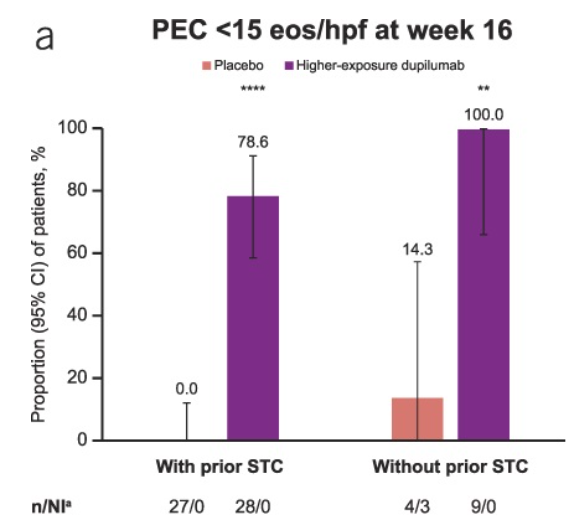
- At W16, higher-exposure dupilumab improved rates of histologic remission vs placebo in patients with prior STC use (60.7% vs 0.0%) and prior IRIC to STCs (60.9% vs 0.0%).
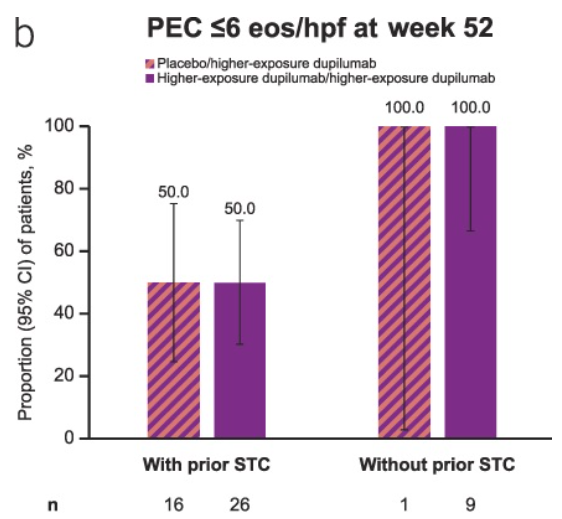
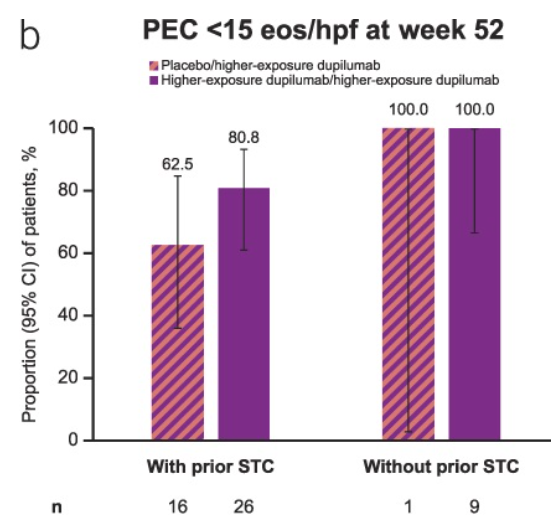
- Responses were maintained at W52 with higher-exposure dupilumab, with improvements observed in patients who switched from placebo to higher-exposure dupilumab.
- “Findings seemed comparable in those without prior STC use or prior IRIC, although patient numbers were small.” Only 9 patients in the treatment cohort did not haver prior STC use.
My take: It appears that dupilumab works well in those with and without prior swallowed topical corticosteroids (STCs). Though the numbers are small, the response appears more robust in those without prior STCs; perhaps, those with prior STC failure had more refractory EoE.
Some good brief YouTube EoE educational videos for families from GIKids.org (with pharmaceutical funding), links:
- Are you having trouble swallowing? (3 minutes)
- My Child Chokes When He Eats (1 minute)
Related blog posts:
- Dupilumab (Dupixent) for Young Children with Eosinophilic Esophagitis (Published Data)
- Dupixent Approved in Younger Children (15 kg+)
- “Real-World” Dupilumab for Eosinophilic Esophagitis
- Practical Tips for Eosinophilic Esophagitis
- Misleading Study on Topical Steroids for Eosinophilic Esophagitis -Comparing Four Apples to One Apple
- Extent of Eosinophilic Esophagitis and Response to PPI Therapy
- The Esophagus Works Better After Responding to Treatment for Eosinophilic Esophagitis
- Updated Data on PPI Effectiveness For Eosinophilic Esophagitis
- Is Topical Budesonide Less Effective in Patients With Eosinophilic Esophagitis With Strictures?
- Long-Term Treatment of Eosinophilic Esophagitis with Budesonide