M Abu-El-Haija et al. Clinical Gastroenterology and Hepatology, 2026. (Article in print). DOI: 10.1016/j.cgh.2026.06.004. Open Access! Pancreatitis Risk Genes Play a Major Role in Pediatric Pancreatitis: Insights From INSPPIRE
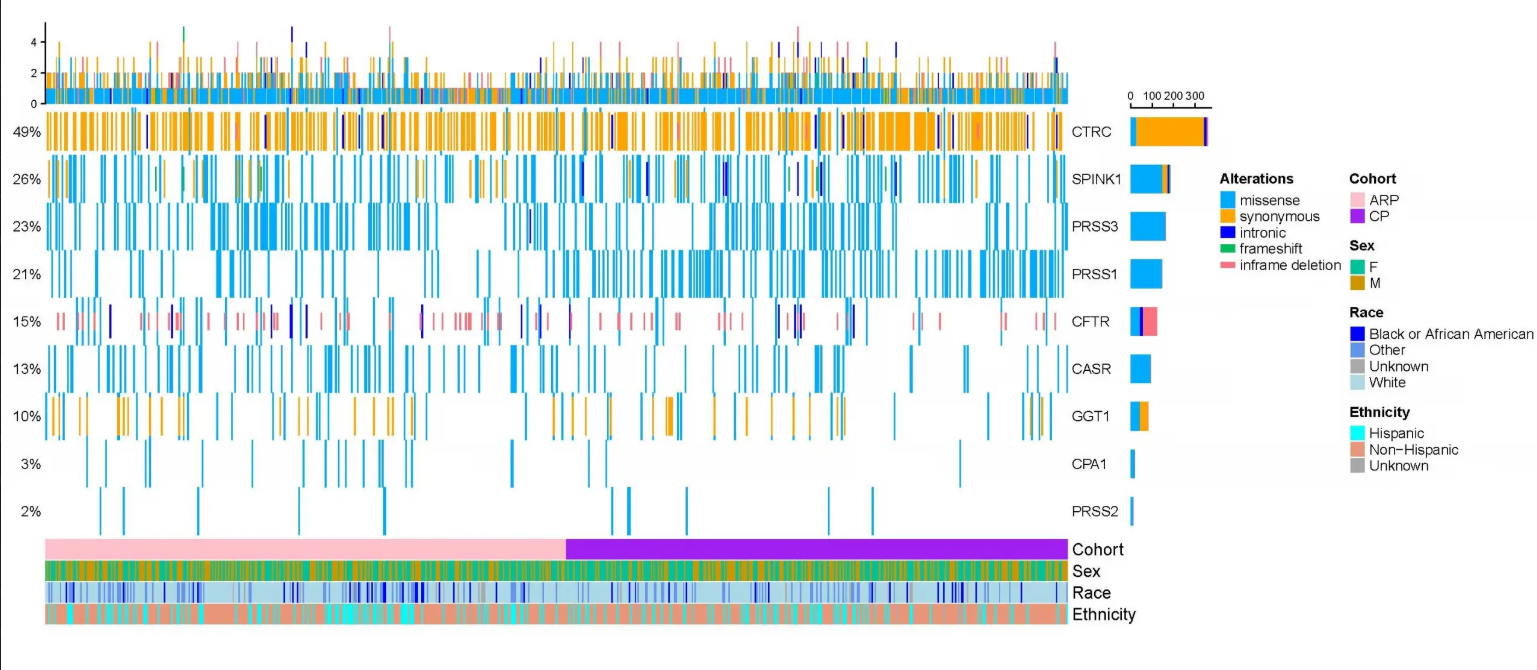
Methods: A cross-sectional study involving 944 pediatric ARP or CP subjects was conducted. CASR, CEL, CFTR, CLDN2, CPA1, CTRC, GGT1, PRSS1, PRSS2, PRSS3, SBDS, SLC26A9, SPINK1, and UBR1 were sequenced.
Key findings:
- A total of 120 variants, including 79 never previously reported to be associated with pancreatitis.
- 38 focused variants found in CFTR (10 variants), PRSS1 (6), CTRC (6), SPINK1 (5), PRSS3 (3), GGT1 (3), CASR (2), CPA1 (2), and PRSS2 (1).
- Seventy-four percent of children with acute recurrent pancreatitis (ARP) and chronic pancreatitis (CP) carried at least one genetic risk variant.
- In CP, CTRC (p=0.012) and PRSS1 (p<0.001) variants were most common. The presence of any genetic risk variant was associated with faster disease progression from AP to CP compared to none (p=0.014).
My take: This study shows the essential role that genetic mutations have in increasing the risk of ARP or CP. It reinforces the need for genettic testing in children with more than one episode of acute pancreatitis.
Related blog posts:
- Kids With Acute Pancreatitis Need Followup
- Here’s the Data: Endocrine Insufficiency After Acute Pancreatitis in Children
- How to Upgrade Pancreas Care –Jay Freeman MD (Part 1)
- How to Upgrade Pancreas Care –Jay Freeman MD (Part 2)
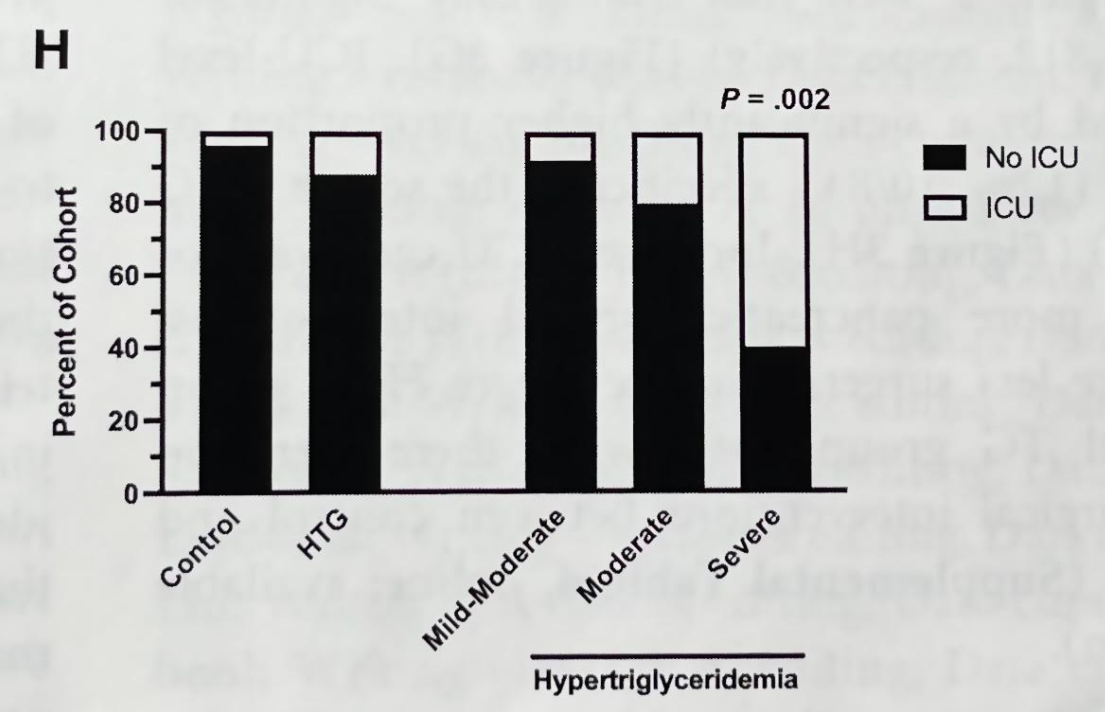
- How Triglycerides Affect Outcomes in Pediatric Pancreatitis
- Diabetes Mellitus Associated with Acute Recurrent and Chronic Pancreatitis
- Likelihood of Genetic Disease with Early-Onset Pancreatitis