N Patel et al. JPGN 2021; 72: 144-150. full text Endoscopic Pancreatic Function Testing (ePFT) in Children: A Position Paper From the NASPGHAN Pancreas Committee
This articles serves as a good review of exocrine pancreatic insufficiency (EPI).
Etiologies:
- “Cystic fibrosis is the most common cause of EPI in children .” Other congenital causes include aberrant embryonic development of the pancreas, “Shwachman-Diamond syndrome, Johanson-Blizzard syndrome, Pearson marrow pancreas syndrome, and Jeune syndrome”
- “Acquired causes of EPI can be transient, such as in the aftermath of acute pancreatitis (which can persist weeks to months)”
- Also, infants, compared to adults, have “physiological” EPI. Lipase output is 5–10% of adult values during the 1st 6 months of life.
Advantages/Disadvantages of Endoscopic Testing for EPI:
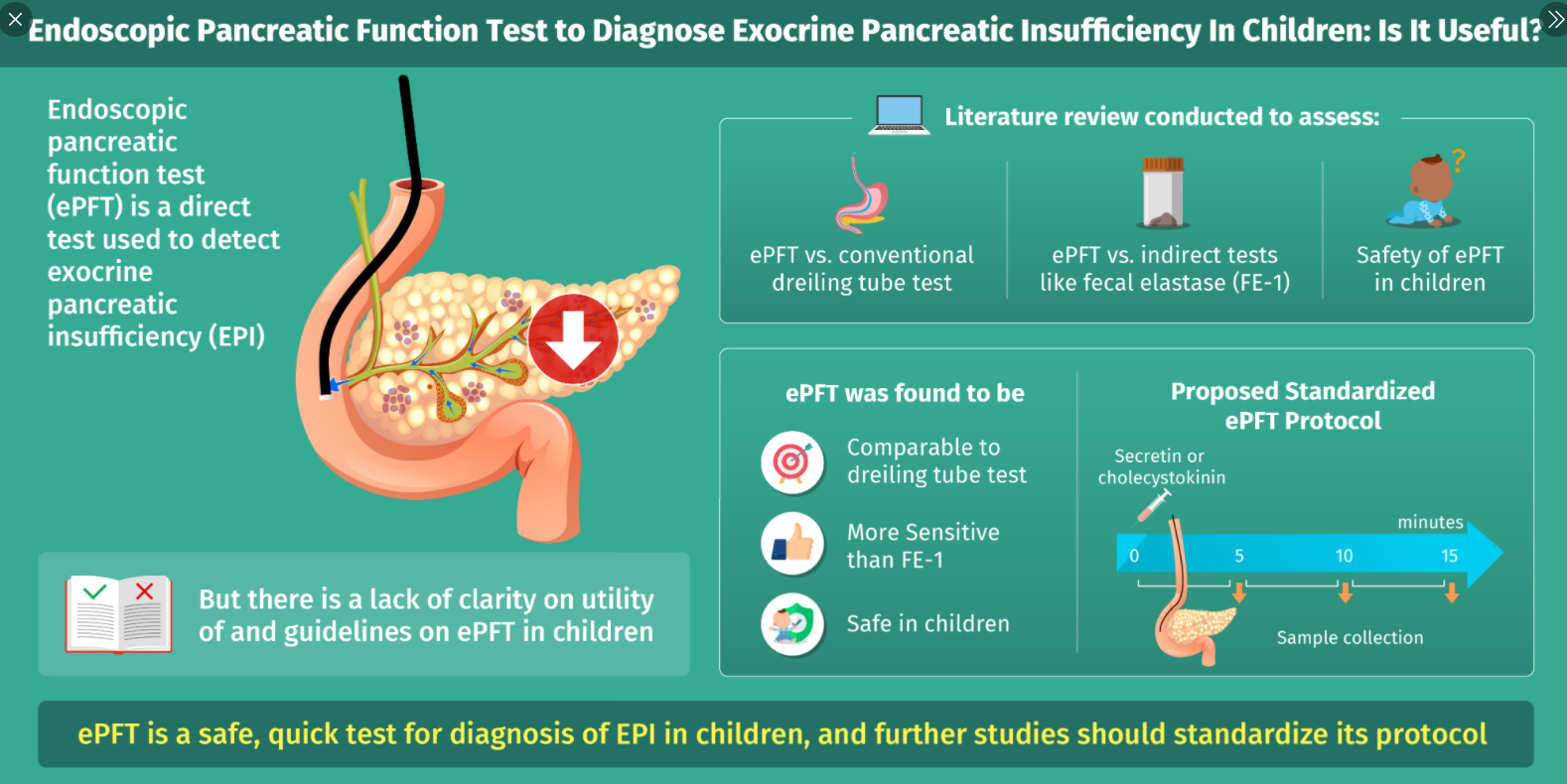
- Advantages:
- • Safe, technically easy, and quick procedure to perform in conjunction to routine investigative EGD
- • Allows assessment of acinar and ductal function
- • High sensitivity and specificity in detection of isolated and generalized enzyme deficiencies
- • Can diagnose minor and more severe degrees of EPI and aid in early diagnosis of CP in patients with unremarkable radiological changes
- Disadvantages:
- • Can be done only in conjunction with EGD and the patient will likely require sedation• Prolongs routine EGD
- • Assesses peak enzyme activity and bicarbonate concentrations rather than total secretory capacity
- • No standardized pancreatic fluid collection frequency or duration in pediatrics
- • Lack of age-specific standardized reference ranges in pediatrics
Endoscopic Testing Caveats:
- Any sample with a pH less than 7 may be unreliable as it is below the pH optimum of the enzymes and may reflect contamination with gastric fluid; however, ” the inability to increase pH, or bicarbonate, upon secretin stimulation may be reflective of loss of cystic fibrosis transmembrane conductance regulator (CFTR) function”
- Samples need to be frozen or placed on dry ice
- “Commonly used laboratory (Kaleida Health Children’s Hospital Laboratory, Buffalo, NY) are: trypsin >55.4 nmol · mL−1 · minute−1, amylase >32 μmol · mL−1 · minute−1, lipase >146 μmol · mL−1 · minute−1, and chymotrypsin >2.5 μmol · mL−1 · minute−1“
My take: With careful clinical judgement, endoscopic EPI testing is rarely needed. First of all, fecal elastase measurements can detect most patients with EPI. In addition, a lot of patients with poor growth and suspected malabsorption are too young for reliable endoscopic EPI testing.
Related blog posts:
- Transient Exocrine Pancreatic Insufficiency or Misleading Tests?
- How Helpful is Endoscopic Pancreatic Testing in Pediatrics? | gutsandgrowth A protocol for endoscopic EPI testing detailed in this post
- Fluctuating Elastase Levels in Infants with Cystic Fibrosis