R Rosen et al. Gastroenterol 2026; 170: 1347-1366. Open Access! Rome V Pediatric Upper Gastrointestinal Disorders of Gut-Brain Interaction
This article has a lot of useful information and I recommend reading the article in full. The two previous days, the blog posts reviewed Esophageal Disorders and Functional Pediatric Feeding disorders. Today’s covers gastrduodenal disorders, including the following:
Gastroduodenal Disorders
- Rumination Syndrome
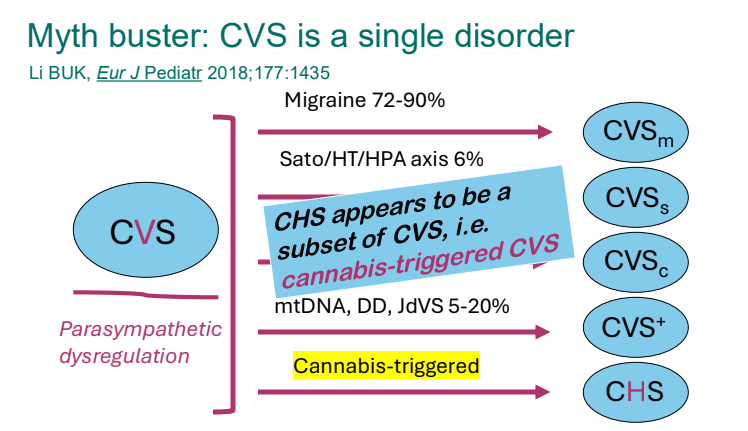
- Cyclic Vomiting Syndrome
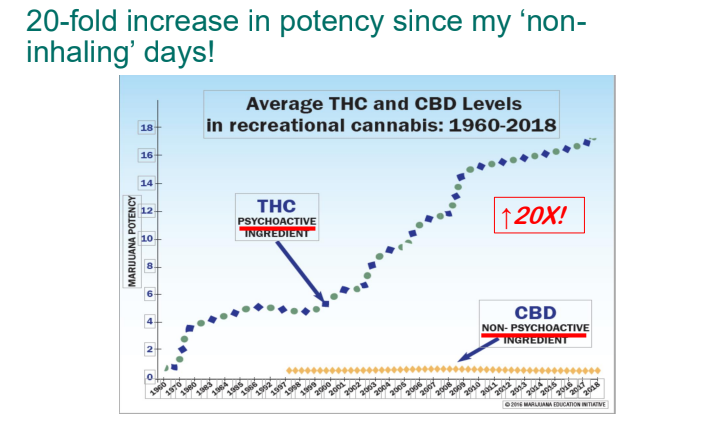
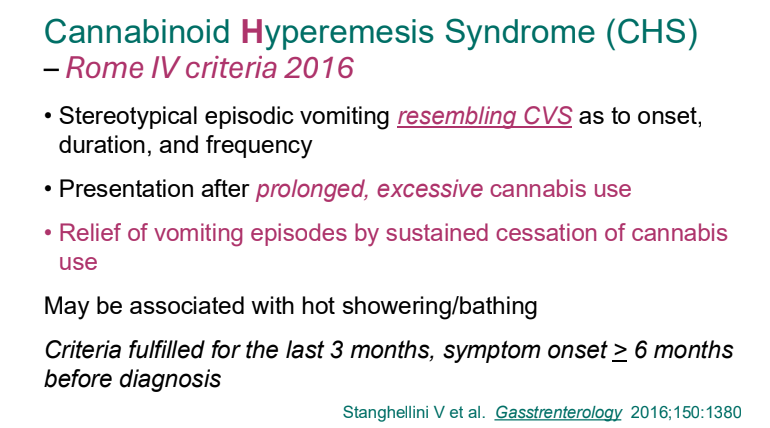
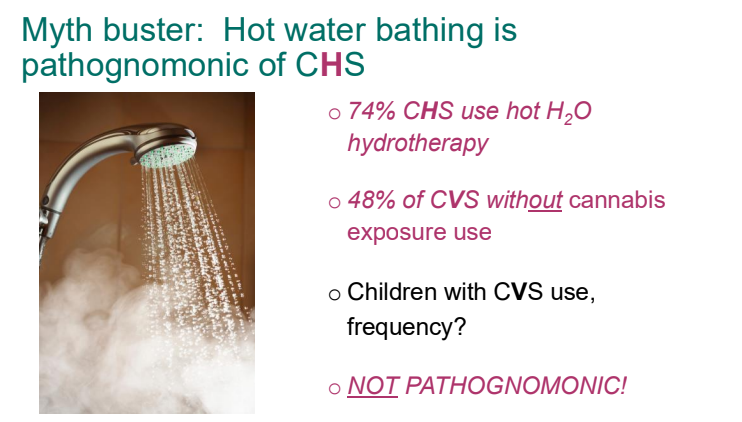
- Cannabinoid hyperemesis subgroup
- Chronic Nausea
- Functional Dyspepsia
- Postprandial Distress Syndrome
- Epigastric Pain syndrome
The key points:
Rumination syndrome: “The revised criteria require lack of response to GERD treatment—or, in infants, troubling regurgitation—before diagnosing RS…Delayed gastric emptying is seen in up to 45% of pediatric RS cases.106…Clinical observation during or after meals is often sufficient for diagnosis.111 Confirmatory tests, such as HRIM (R-wave), 24-hour pH-impedance monitoring, or upper endoscopy and contrast studies may be needed for atypical presentations or when there is diagnostic uncertainty.109,112,113…In older children, up to 70% of children have at least 1 psychiatric comorbidity.109,110 Anxiety, depression, and eating disorders are most common, although attention-deficit hyperactivity disorder, obsessive-compulsive disorder, and adjustment disorder have been reported.111
Treatment of rumination syndrome: “23% of children diagnosed with RS showed self-resolution of symptomatology without treatment after only the initial counseling.115 … The treatment in older children and adolescents focuses on implementing behavioral strategies, modulating food and liquid intake, managing mental health–related issues, and implementing diaphragmatic breathing around mealtimes.107,116…Baclofen may be an adjunctive therapy, although data in children are limited. A recent retrospective study in children found that baclofen is safe and is effective in almost 50% of children.119“
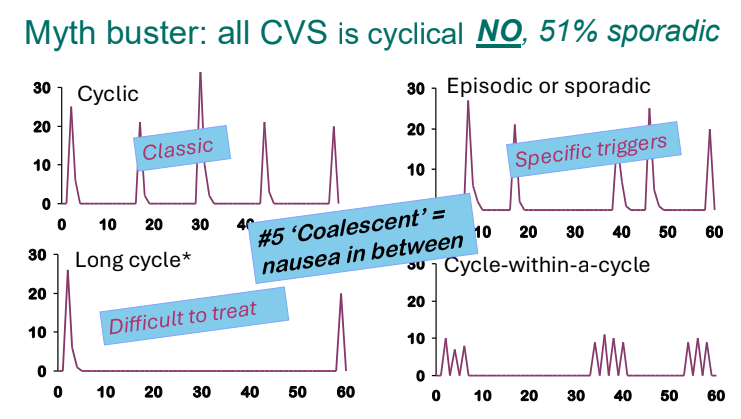
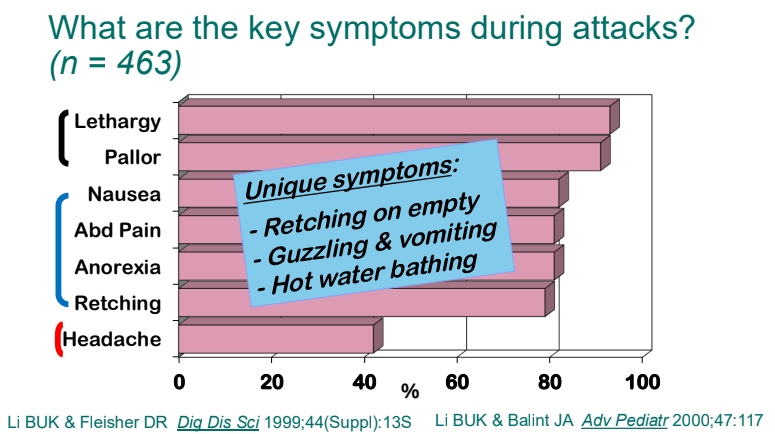
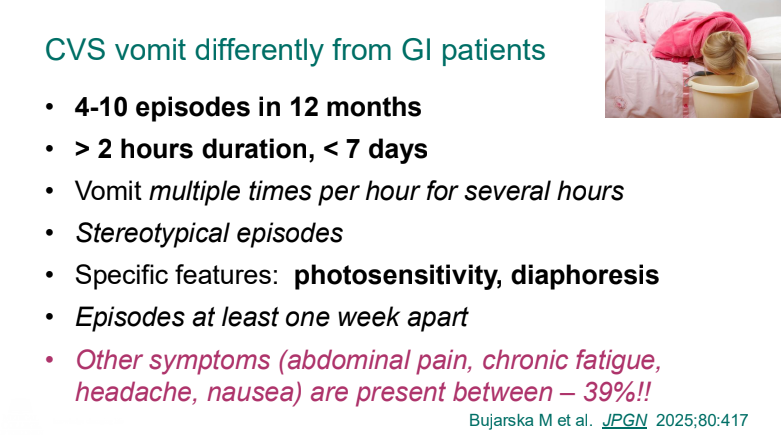
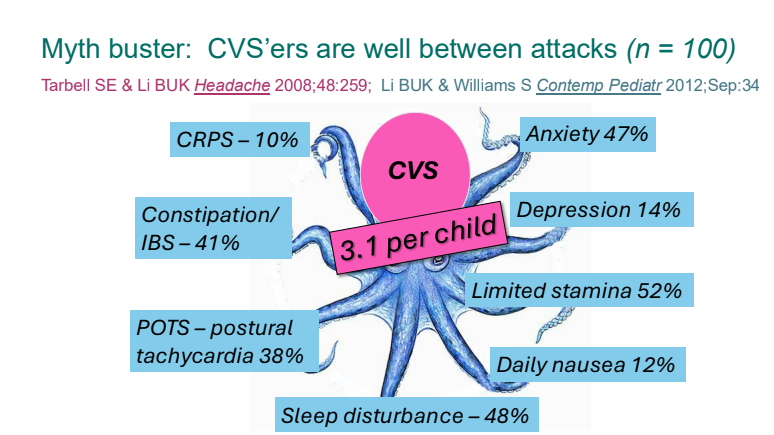
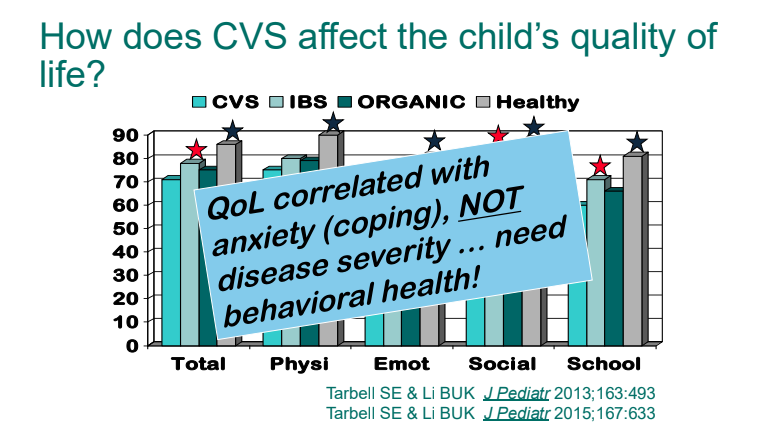
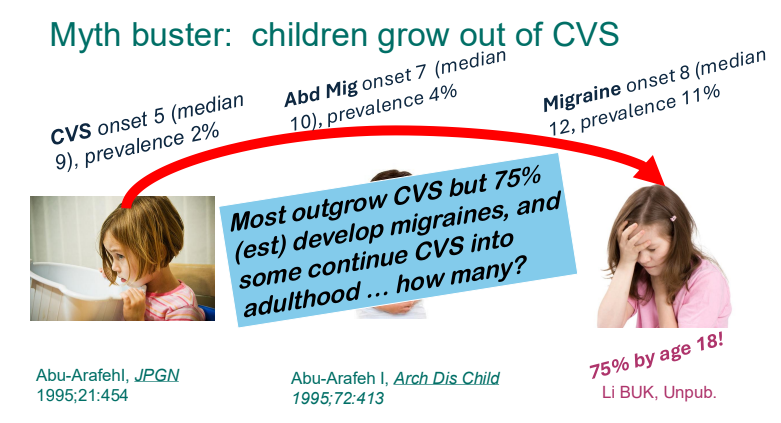
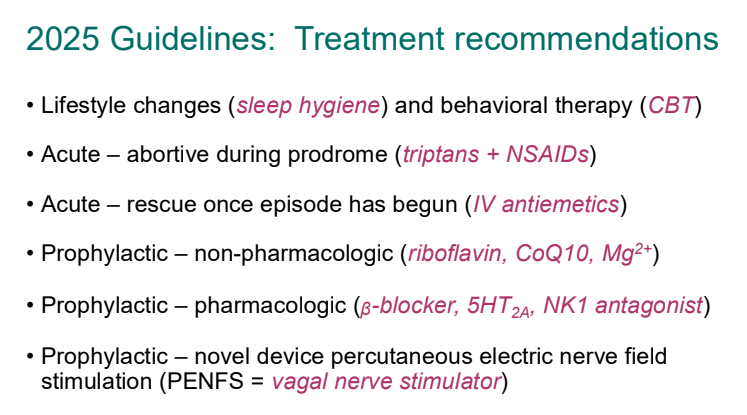
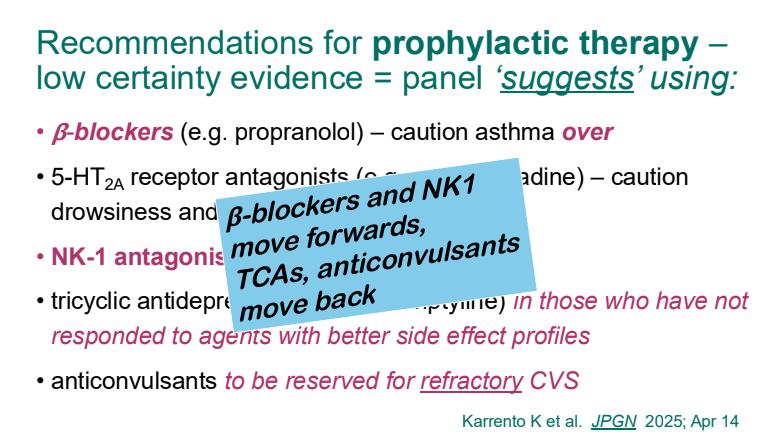
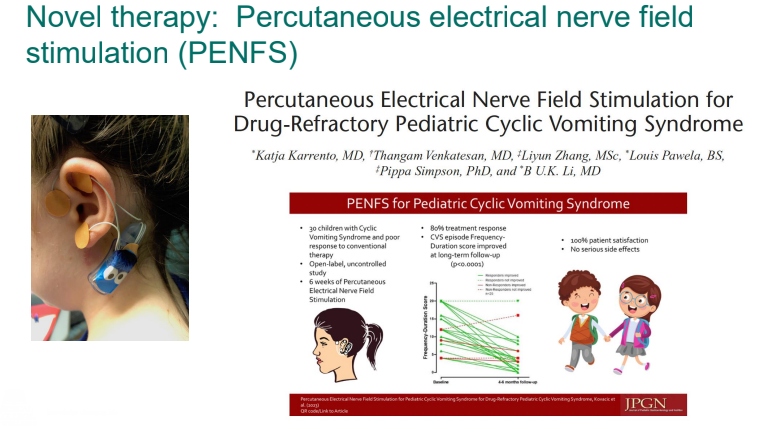
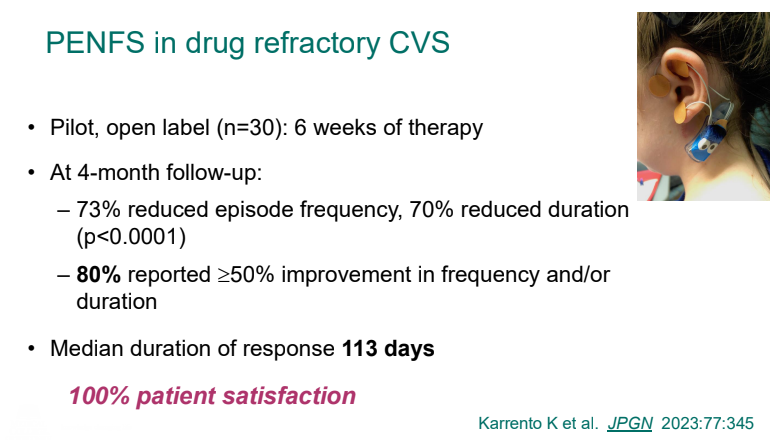
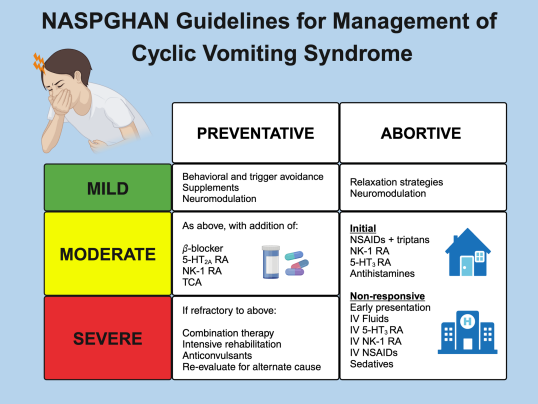
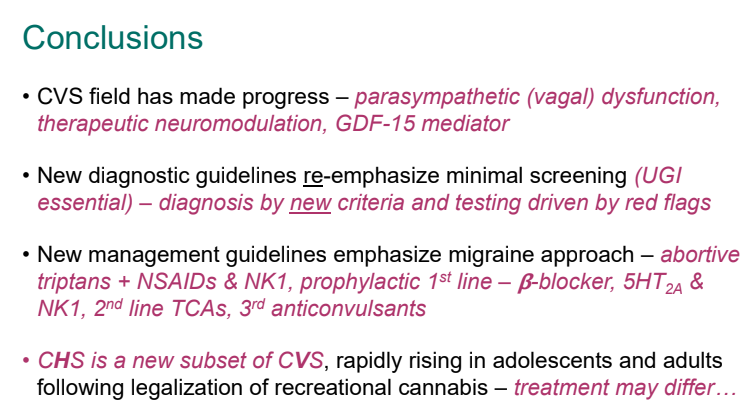
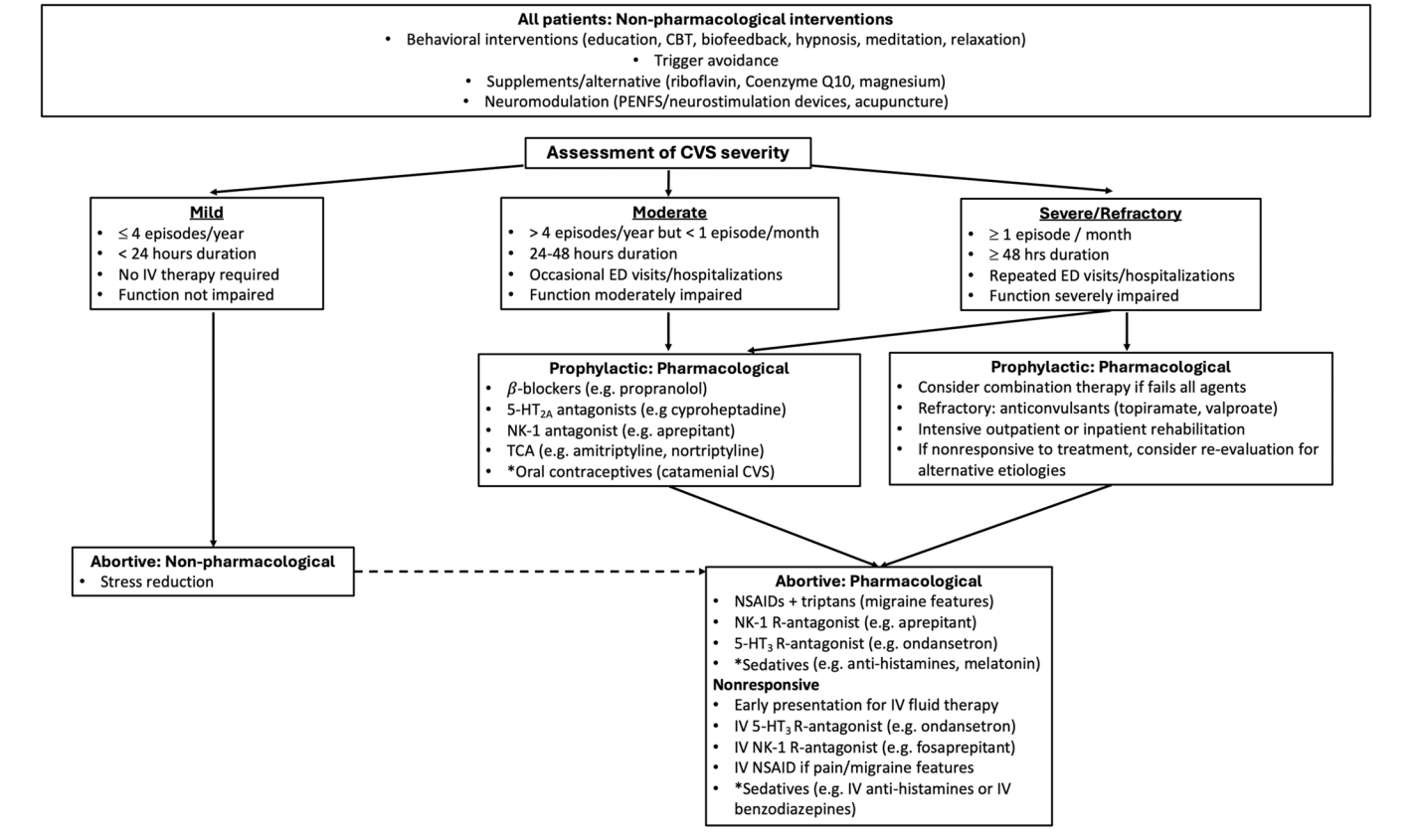
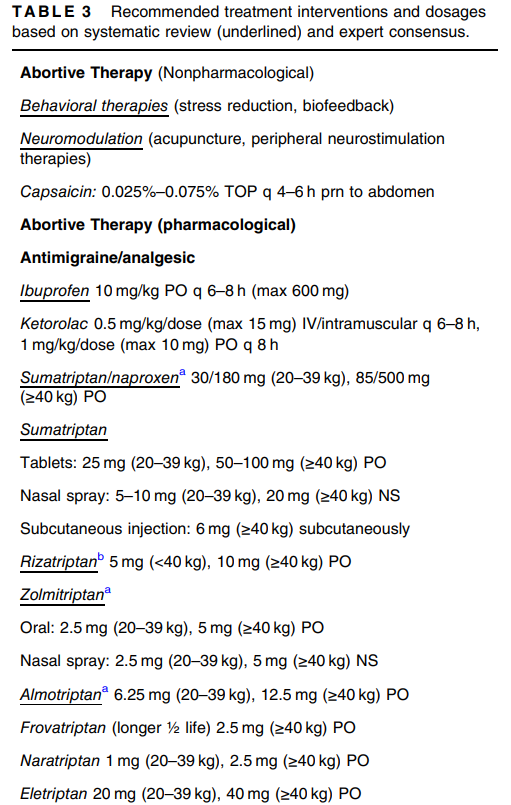
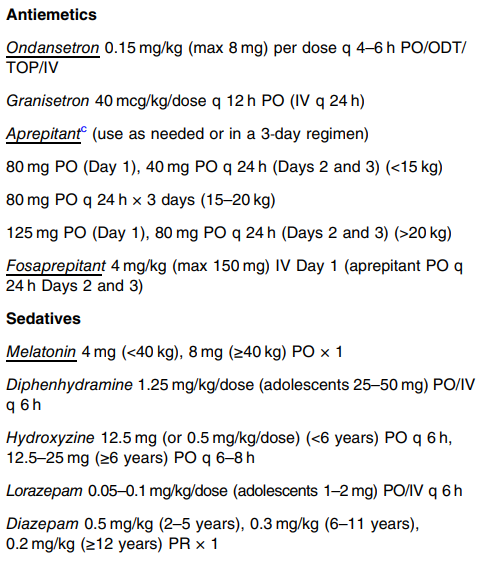
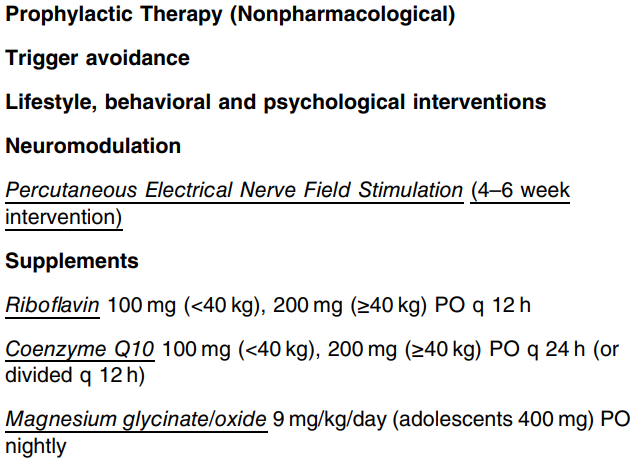
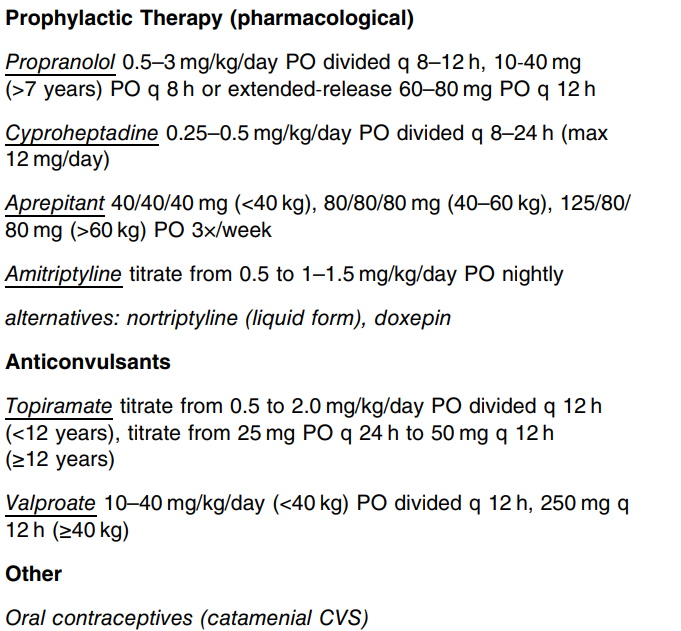
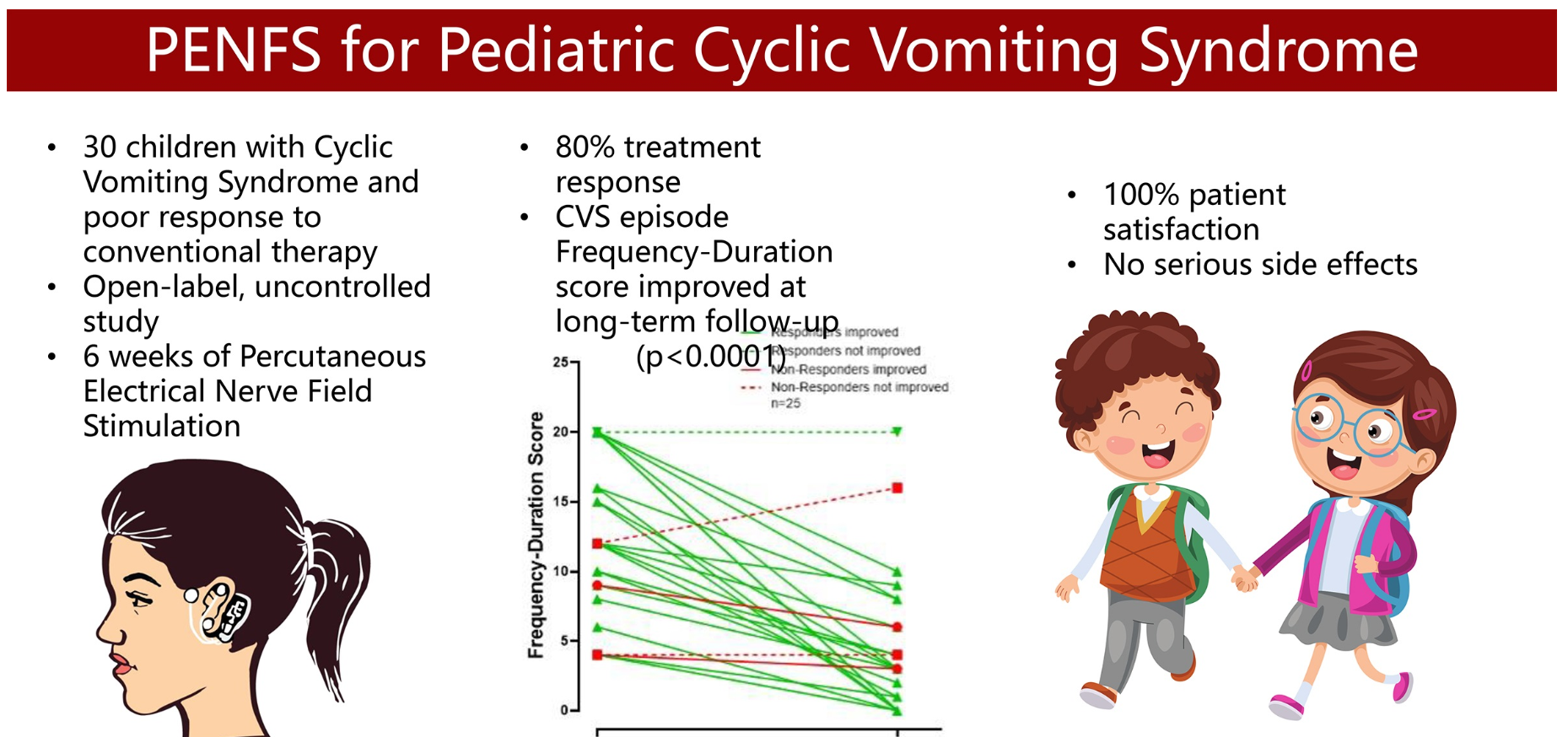
Cyclic Vomiting Syndrome: “CVS leads to significant disability, including an average of 24 missed school days per year and more quality of life impairment than other DGBI.123…The committee supports the treatment approach outlined in the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition CVS guidelines.120“
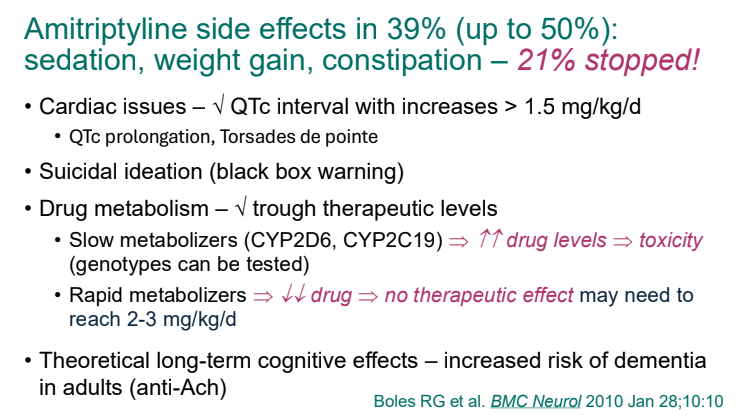
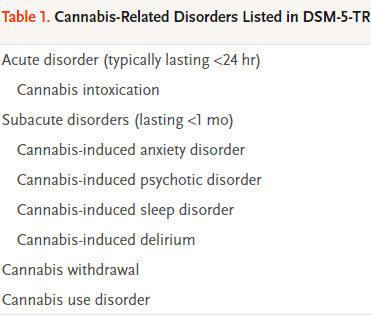
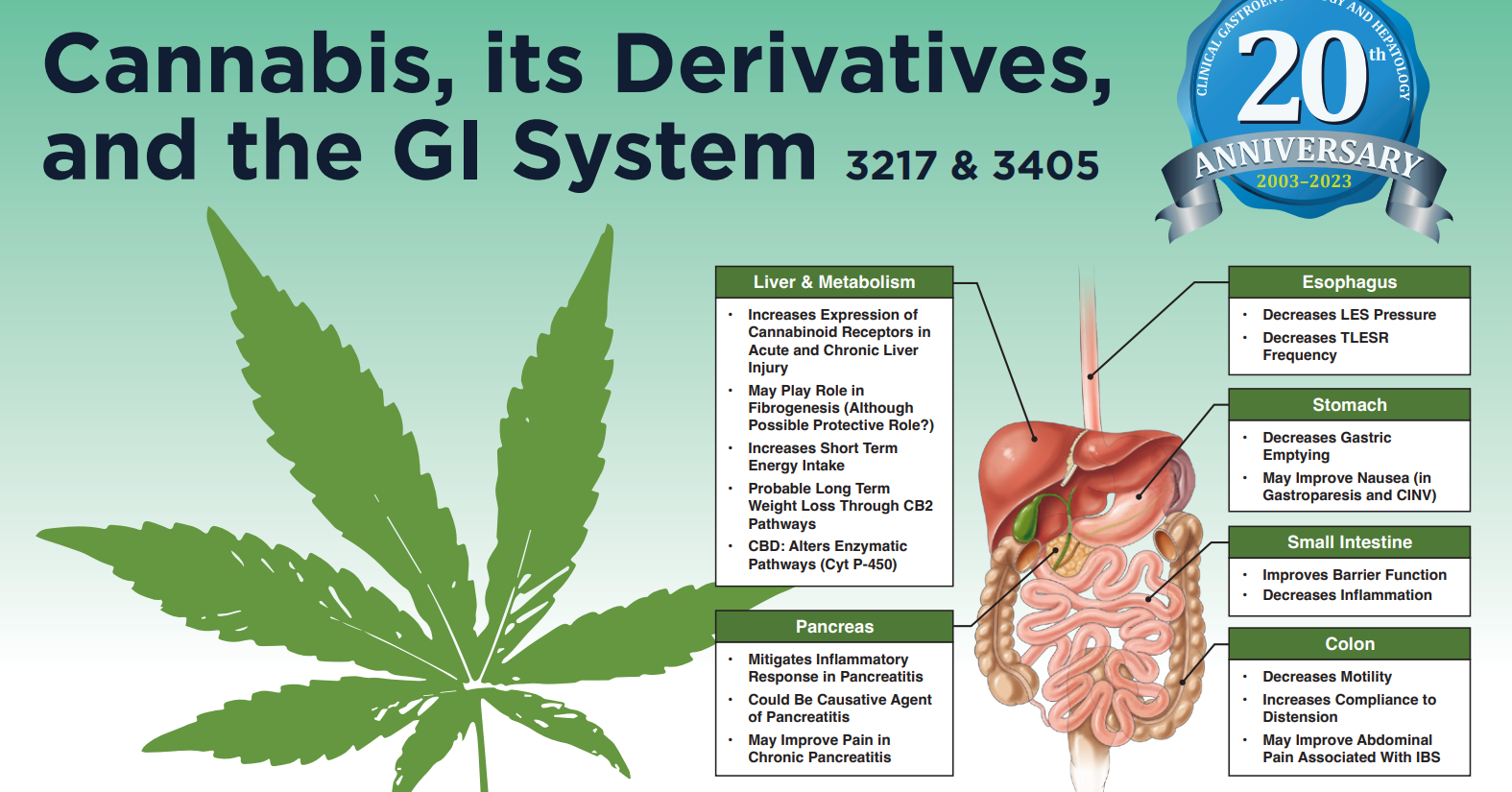
Cannabinoid Hyperemesis Subgroup: “CHS treatment mirrors CVS and includes abortive and preventive therapies.120,132,133 Long-term management centers on cannabis cessation and TCAs like amitriptyline. As sudden cessation may cause withdrawal and relapse, gradual reduction and lower-THC products may improve success.”
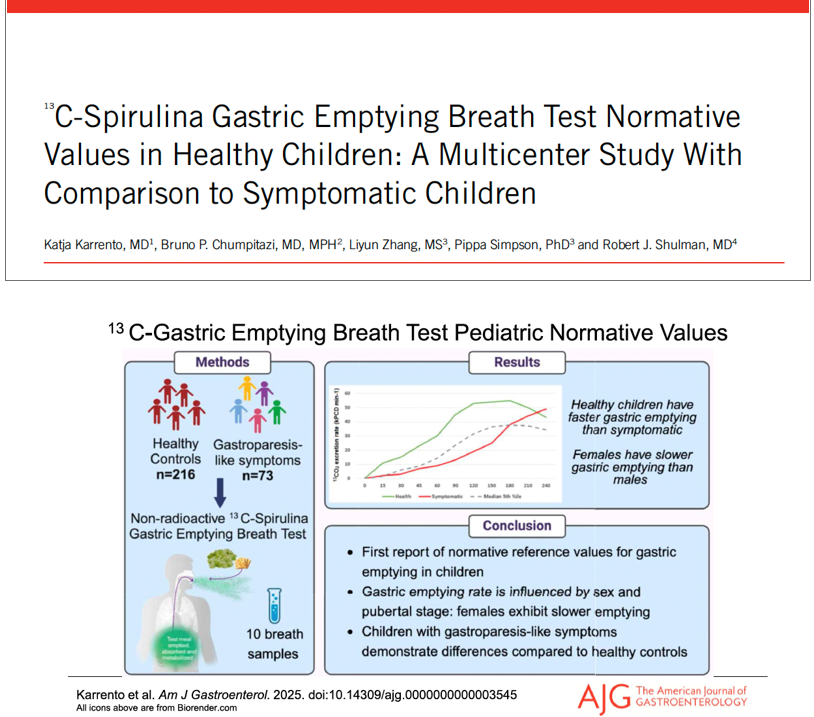
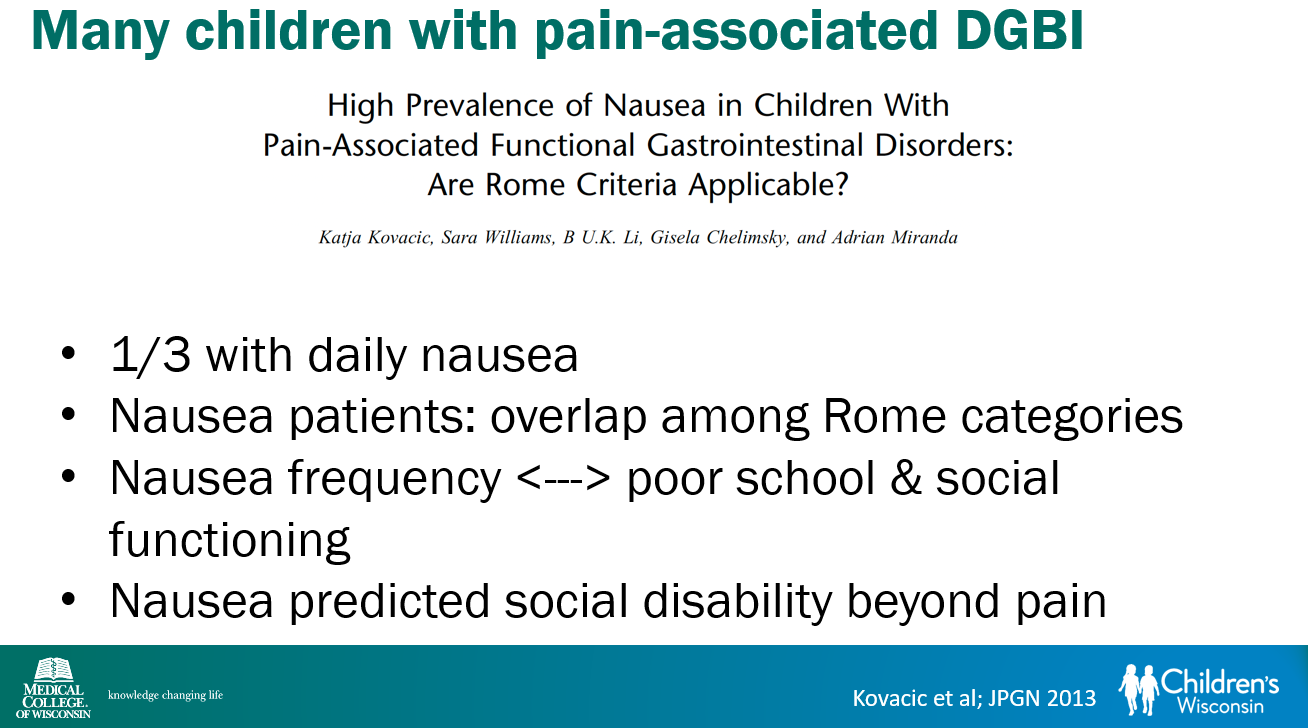
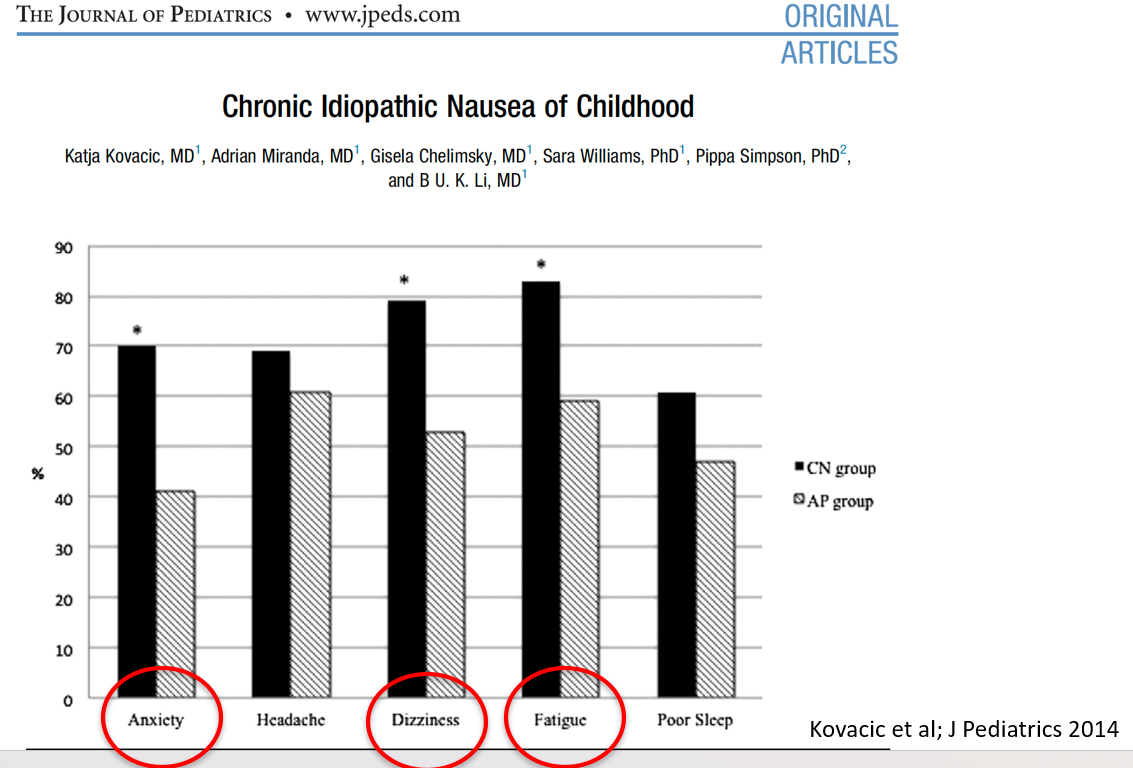
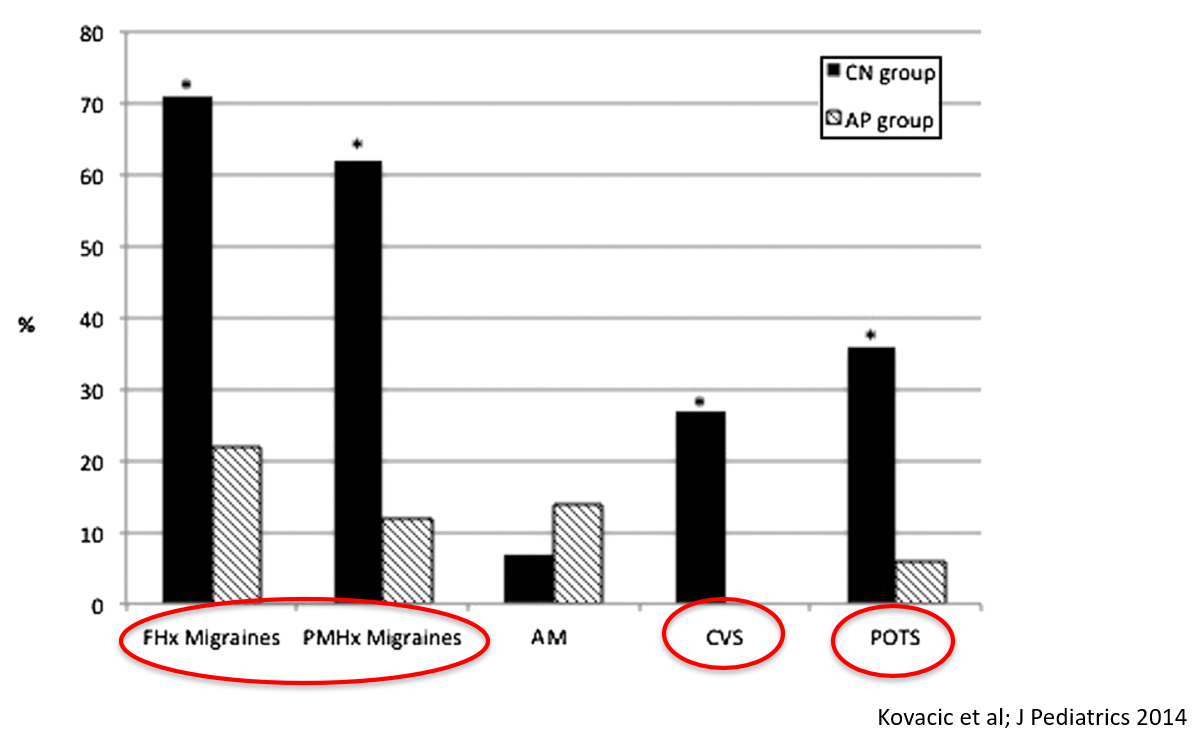
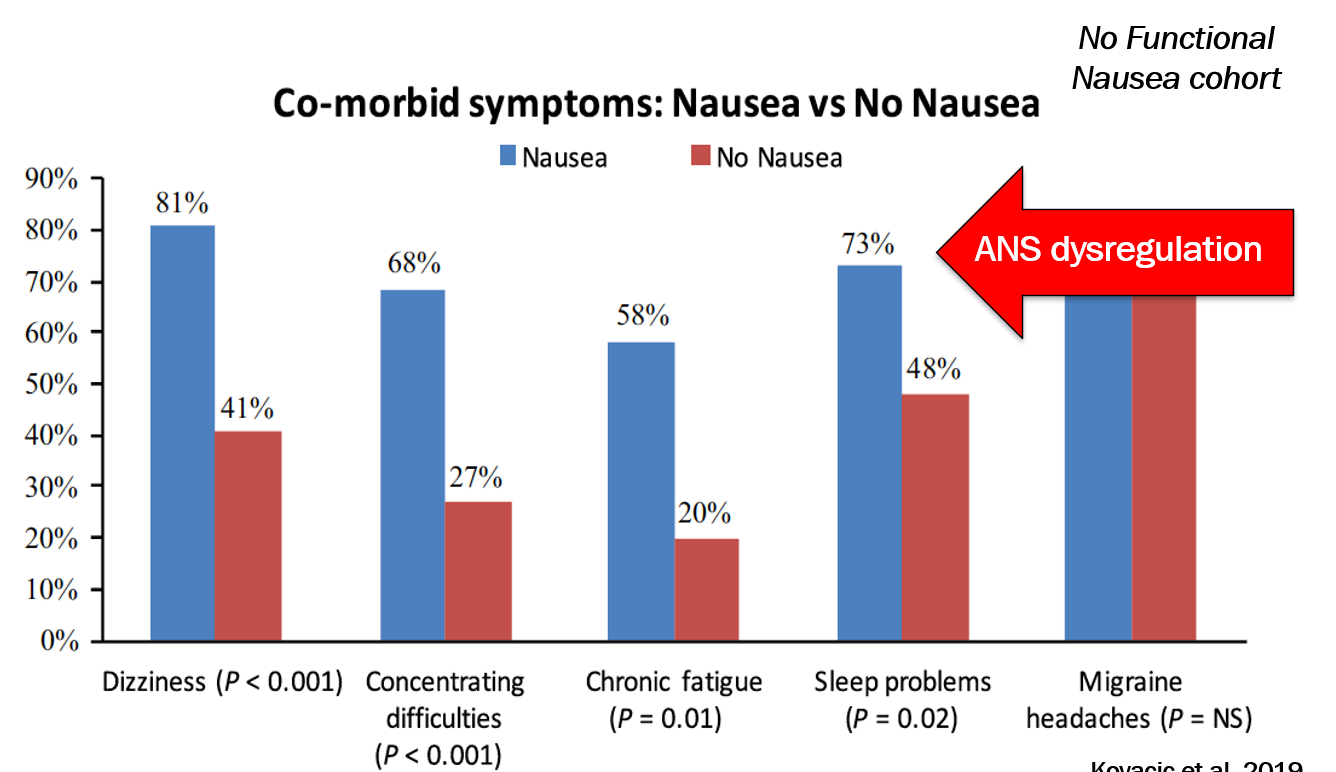
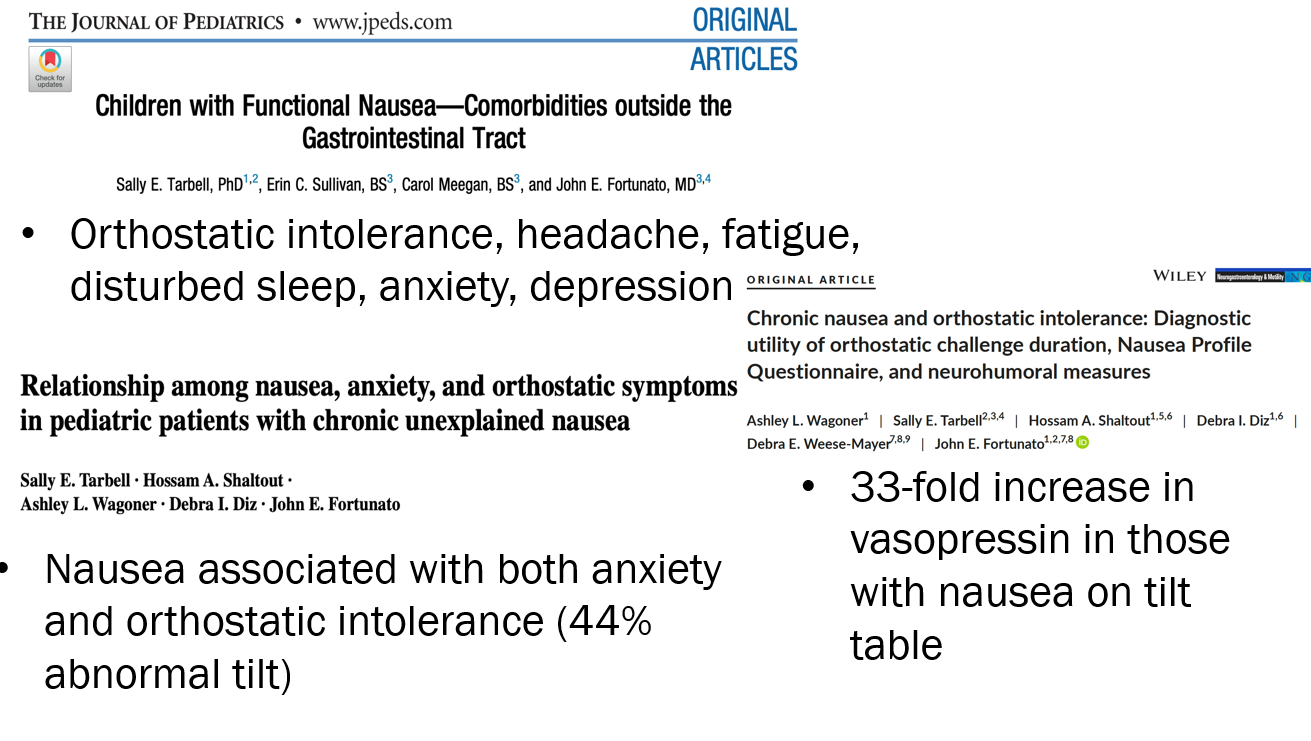
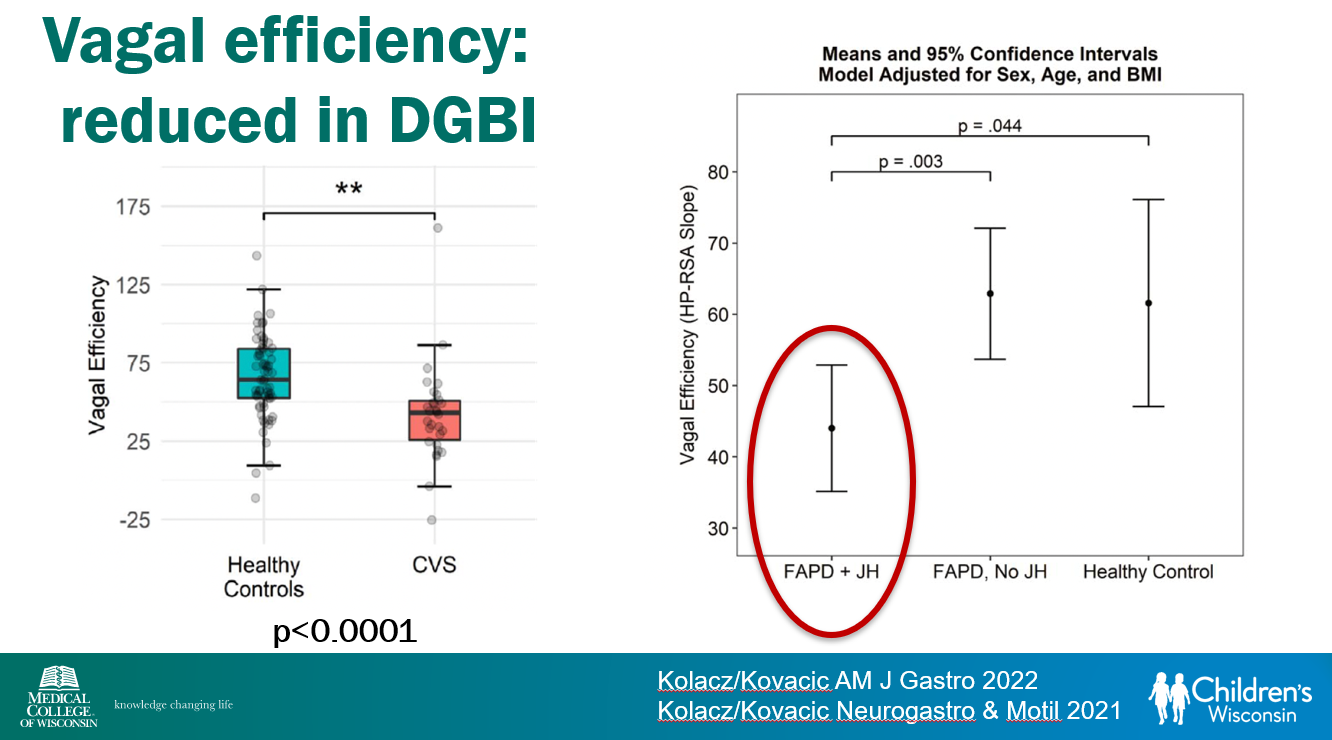
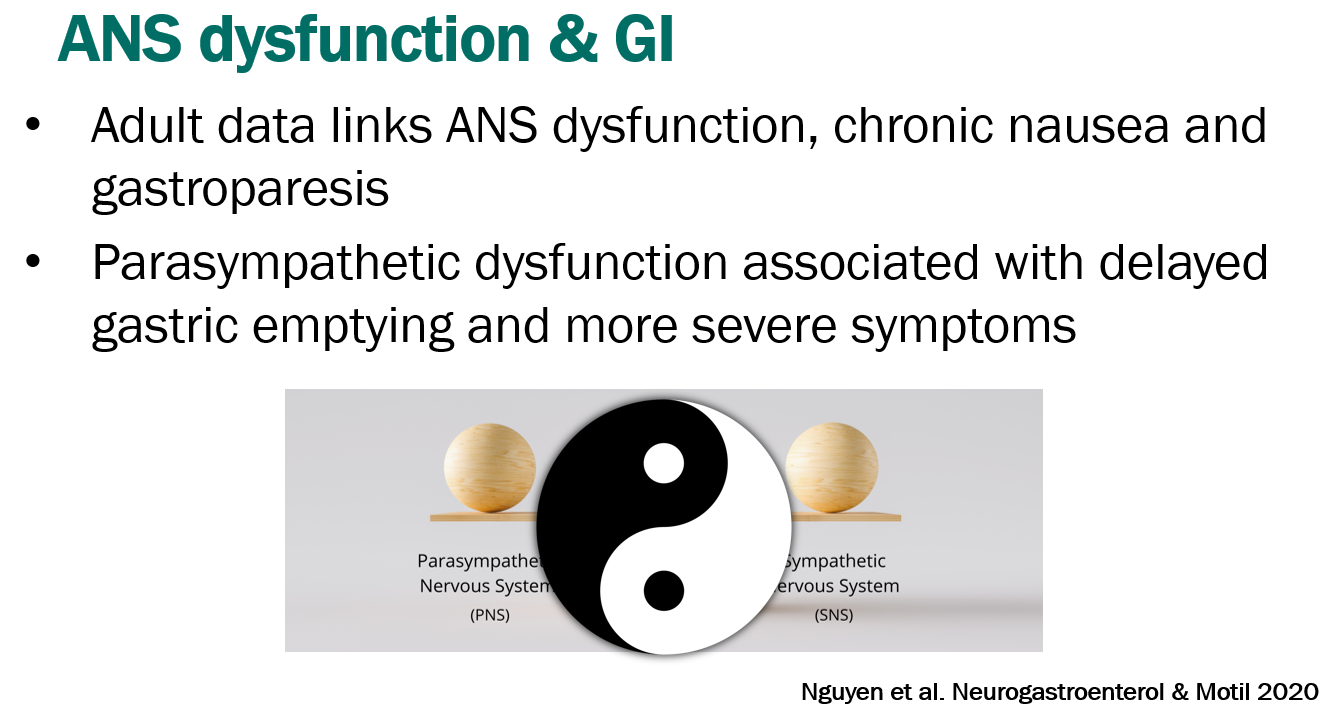
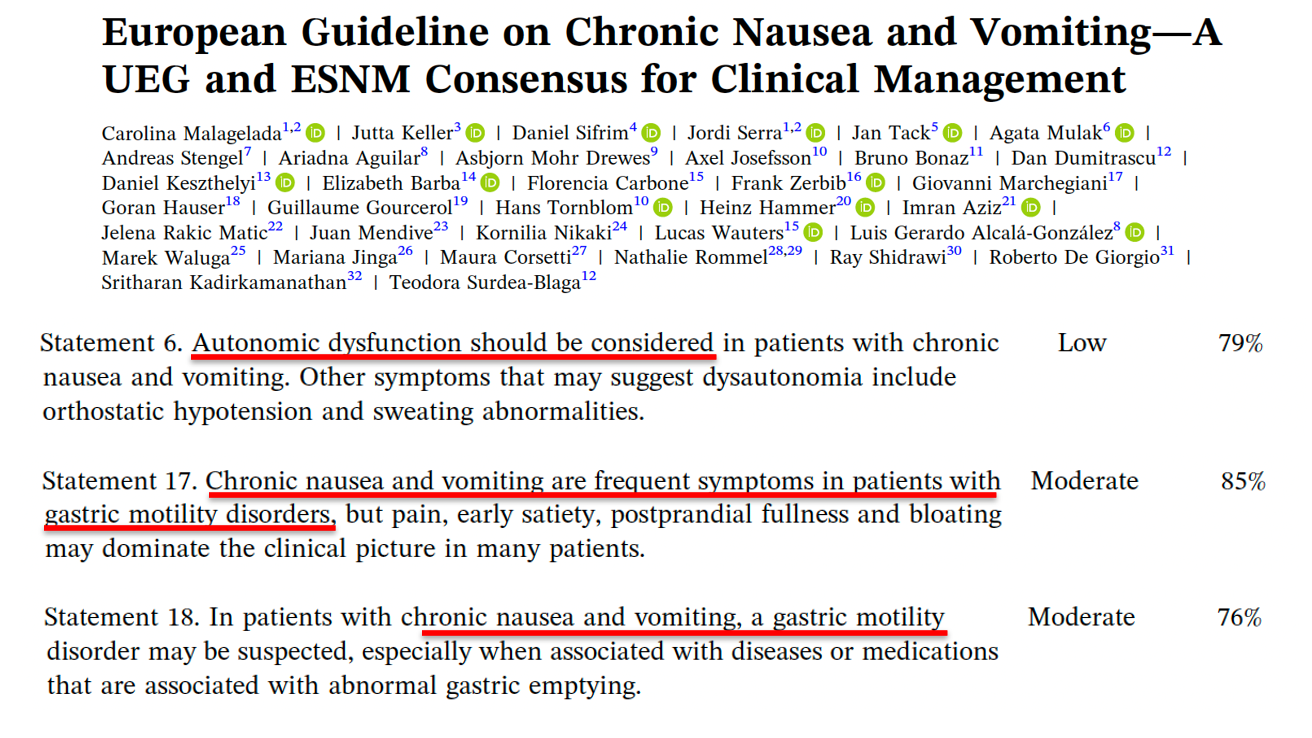
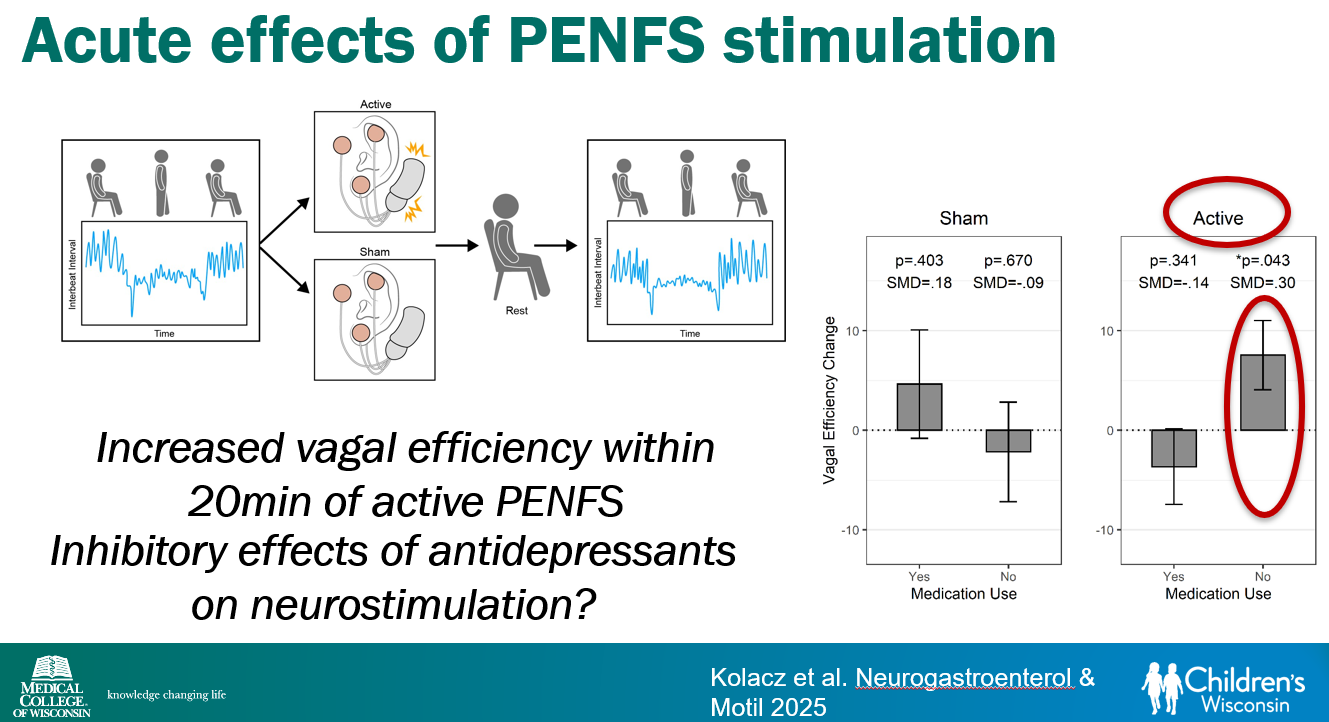
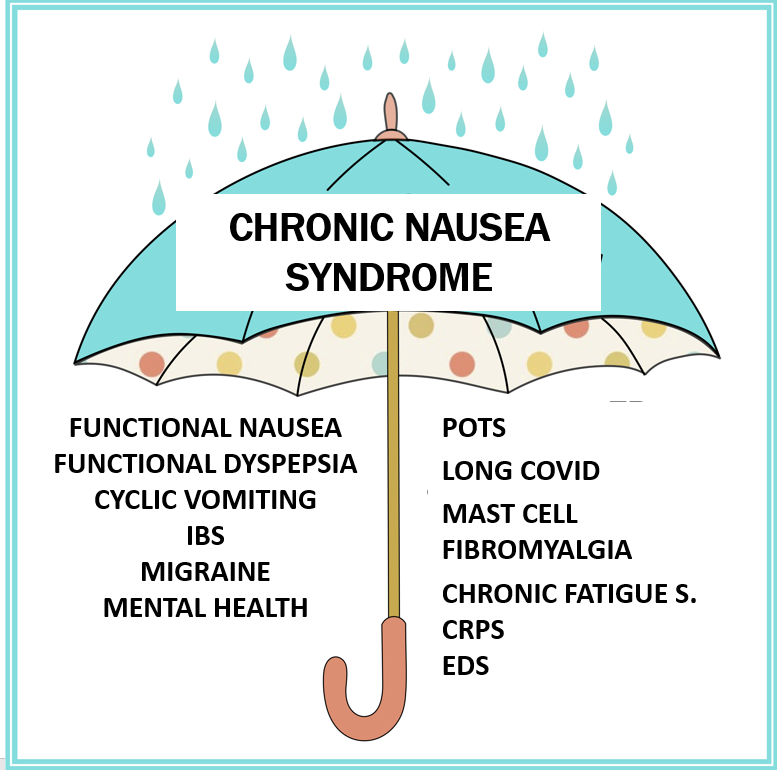
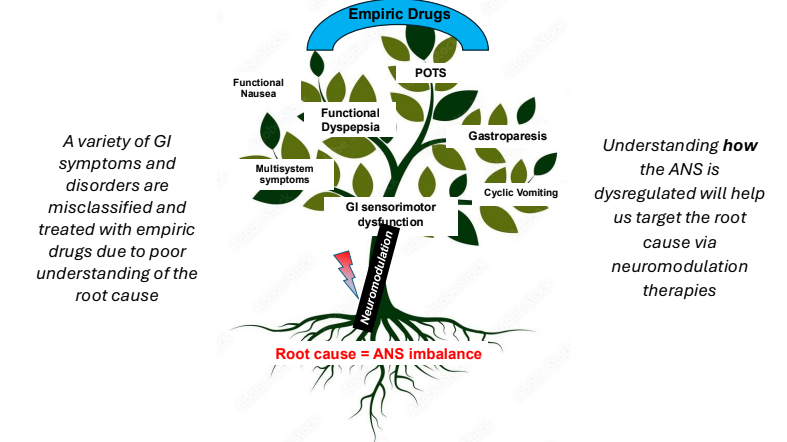
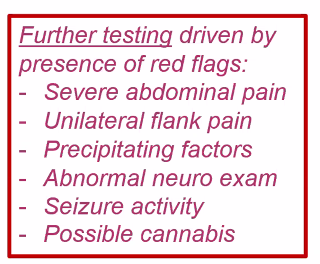
Chronic Nausea Syndrome: “Since its inclusion in Rome IV, studies have confirmed the prevalence of functional nausea and its link to comorbidities like POTS and other autonomic disorders, suggesting it may be part of a broader syndrome. Rome V now uses the term “chronic nausea syndrome” to better reflect this. The diagnostic criteria remain similar to Rome IV. Vomiting is excluded from the definition, as children typically present with nausea alone.” Testing: “routine laboratory tests may be done, but extensive testing rarely provides alternative diagnoses.138 Diagnostic endoscopy is not recommended unless “red flags” are present.138 Gastric-emptying studies are also not routinely needed unless vomiting is severe, the diagnosis is unclear, or the nausea is intractable.”
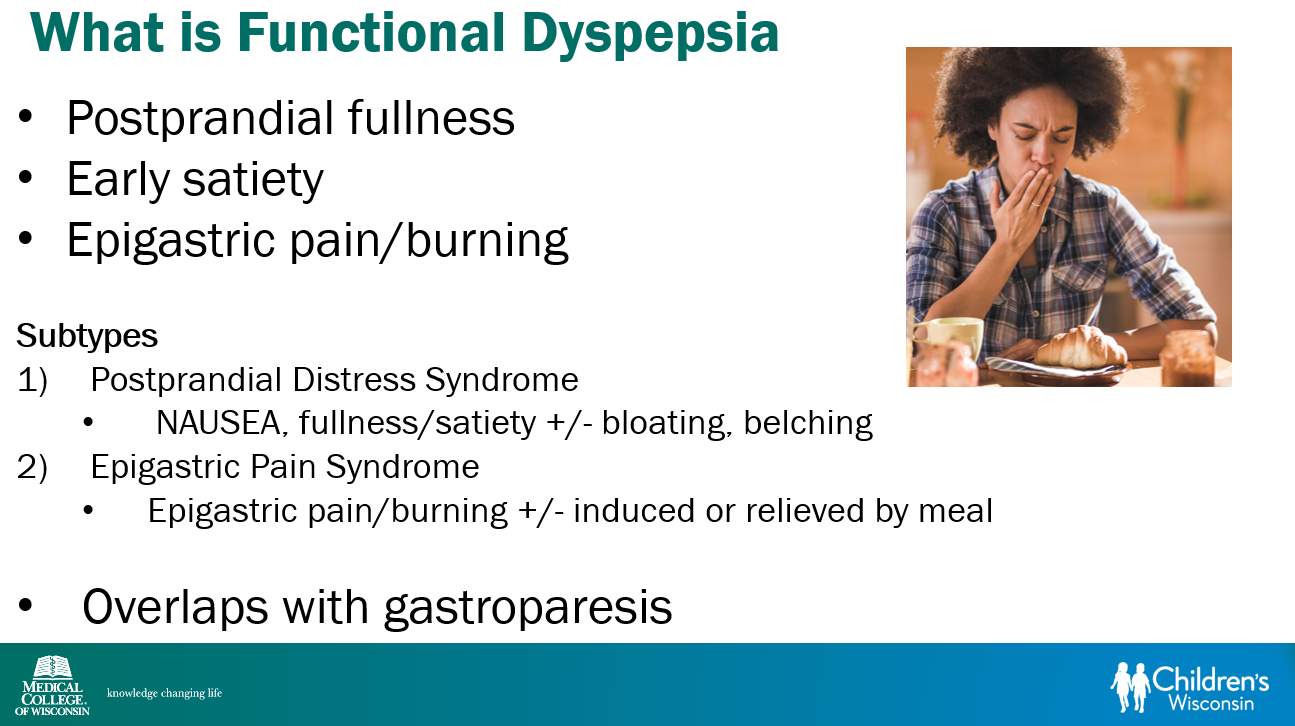
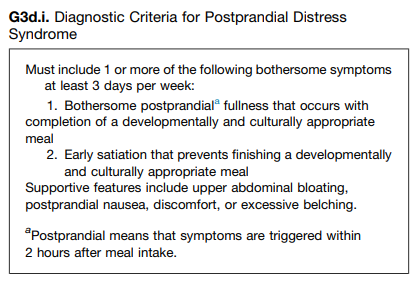
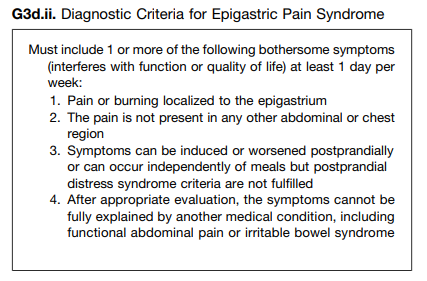
“Function dyspepsia (FD) describes upper GI discomfort that may include a variable combination of features, including epigastric pain, postprandial upper abdominal fullness, early satiety, bloating, nausea, belching, and vomiting. Two main subtypes have been identified: postprandial distress syndrome (PDS) and epigastric pain syndrome (EPS).152–154“
Related blog posts:
- Impact of Testing (or No Testing) for Rumination Syndrome Outcomes
- Potential Bias with Interpreting Rumination Outcomes
- Most Kids with Rumination Respond to Specialized Treatment
- Faulty Narrative with Functional Nausea Study
- Functional Dyspepsia in Clinical Practice
- Dr. Katja Karrento: Chronic Nausea — Evidence of a Complex Syndrome
- Dr. B Li: Cyclic Vomiting Syndrome 2025
- 2025 Pediatric Cyclic Vomiting Syndrome Guidelines
- Is Manometry Useful to Determine if Botox Will Help Nausea/Vomiting?
- Dreaded Nausea (2022) Plus Skills or Pills
- How PPIs Improve Functional Dyspepsia
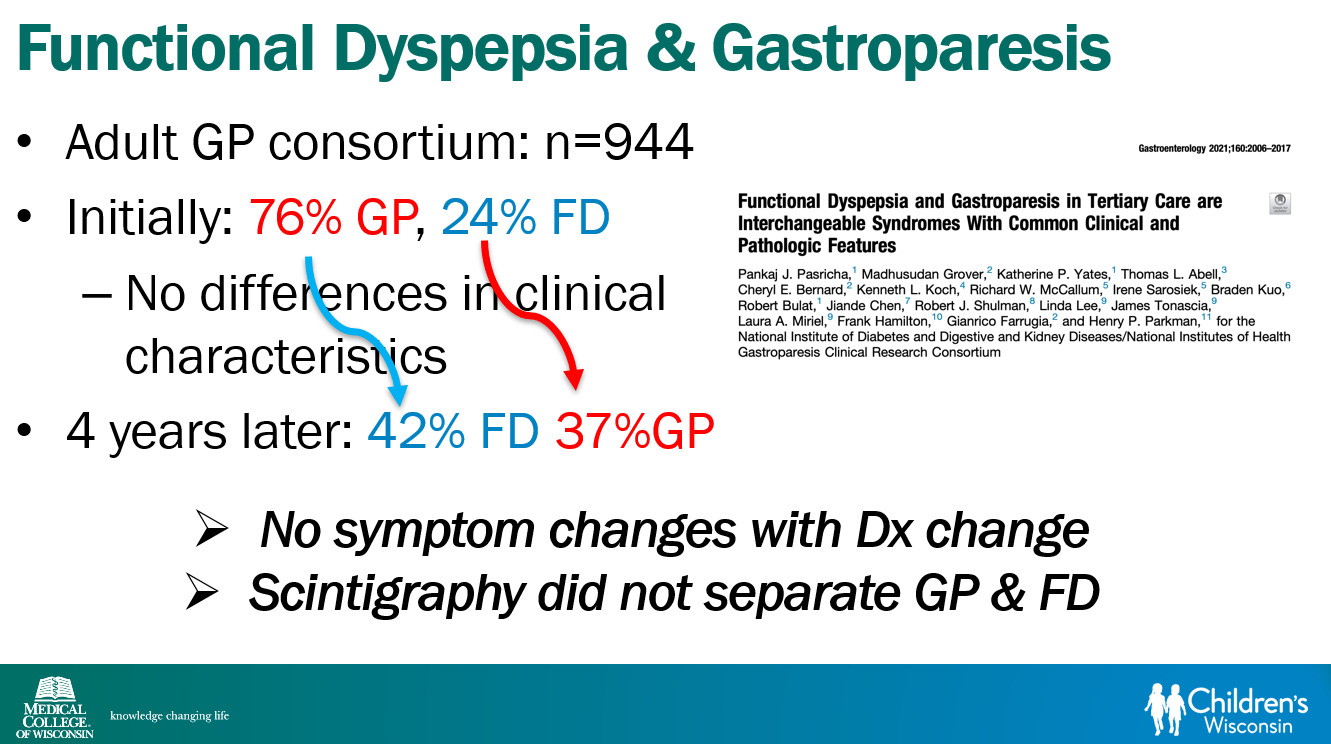
- Are Gastroparesis and Functional Dyspepsia Part of the Same Problem?
- Pregabalin Helpful for Functional Dyspepsia in Small Study
- Mirtazapine for Functional Dyspepsia
- A 6-Year Study of Amitriptyline, Escitalopram, and Functional Dyspepsia