JB Doyle et al. Clin Gastroenterol Hepatol 2026; Risk of solid organ transplantation in individuals with celiac disease: a nationwide cohort study
Background: “Celiac Disease (CeD) is associated with immune-mediated diseases of the liver, including autoimmune hepatitis, primary biliary cholangitis, primary sclerosing cholangitis. Individuals with CeD are also at increased risk for non-autoimmune diseases of the liver, including metabolic dysfunction-associated fatty liver disease…CeD has also been associated with chronic kidney disease and cardiovascular disease. Multiple studies have demonstrated that individuals with CeD have increased rates of end-stage renal disease than the general population, with particularly strong associations between CeD and
autoimmune nephropathy, diabetic nephropathy, and systemic lupus erythematosus (19-22).
Population-level data also suggests that individuals with CeD have an increased risk of
cardiovascular disease and ischemic heart disease>”
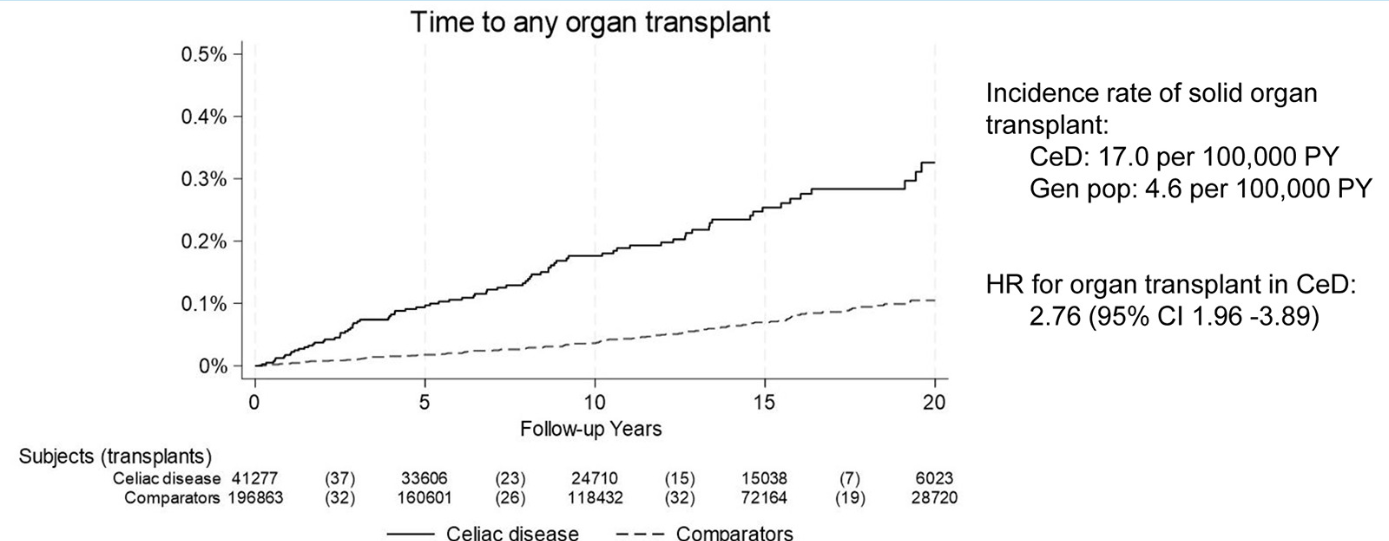
Methods: Population-based matched cohort study in Sweden. We identified individuals with biopsy-proven CeD diagnosed between 2000-2023 using the nationwide histopathology cohort ESPRESSO. We calculated the incidence of solid organ transplantation (liver, heart, kidney, and lung) in CeD patients and estimated the risk relative to the general population. There were 41,277 individuals with CeD and 196,863 age- and sex-matched comparators with a mean follow-up of 12.1 years.
Key findings:
- There were 85 solid organ transplantations in patients with CeD (17.0 per 100,000 person-years) and 111 in matched comparators (4.6 per 100,000 person-years). This corresponded to an adjusted hazard ratio (HR) of 2.76
- The highest relative risk was for liver transplantation: HR 7.26; for kidney HR 1.85. For heart, HR was 2.35 did not reach statistical significance (CI: CI 0.84-6.61)
Discussion:
“Shared genetic susceptibility may explain physiological links between CeD and autoimmune liver disease, especially since we also detected an increase in liver transplantation prior to CeD diagnosis…owever, CeD patients in our analysis had an increased risk of liver transplantation relative to their nonaffected siblings, suggesting that CeD itself may be a risk factor beyond genetic predisposition”
My take: While nearly triple the incidence compared to the general population, the absolute increased risk of needing a solid organ transplant was about 1 in 10,000. For comparison, the risk of dying in a bicycle accident in one’s lifetime is about 1 in 5,000. Nevertheless, it may be worthwhile to screen for CeD in those with end-organ disease. Additionally, checking liver tests periodically in patients with CeD would be reasonable.
Related blog posts: