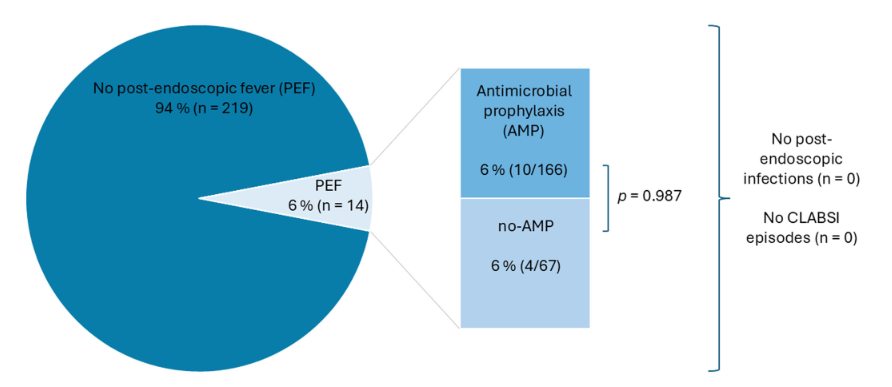
Methods: This was a retrospective single-center observational study which included children with IF and CVC who underwent GI endoscopy between 2019 and 2024. Intravenous antibiotic prophylaxis was used in 71.2% of the procedures.
Key findings:
The overall post-endoscopic fever (PEF) rate was 6%, with no significant difference between the group that received prophylactic antibiotics and the group that did not. Specifically, there were 10 with PEF that had received prophylactic antibiotics and 4 that had PEF with no prophylaxis
No infections, including central line-associated bloodstream infections, were observed
5/14 of the cases with PEF had an interventional procedure. The remainder had a diagnostic EGD, colonoscopy or both.
Interventional Cases:
Discussion Points:
“PEF in children with IF was 6%, which is approximately 10 times higher than the recently published 0.55% in pediatric patients following endoscopic procedures by Boster et al.” (see: Must-Read: How to Handle Post-Procedure Fevers)
A strength of this study was that the comparison of children with IV antibiotics versus those without was due to an institutional policy change in 2022. This helps eliminate selection bias in the determination that IV antibiotics were not beneficial in preventing PEF
My take: The high rate (6%) of PEF should be discussed with families prior to endoscopic procedures. The rate was increased (36%) in those with interventional procedures. It is reassuring that no definitive infections were identified despite the fevers.
From AGA Today (8/5/25): “Sterile Water is Unnecessary for Endoscopy”
GI and Hepatology News (8/4, Pass) reports a review suggests that “endoscopists can safely forgo sterile water in favor of tap, reducing both environmental and financial costs.” Researchers found that only two studies since 1975 “directly compared sterile and tap water use in endoscopy,” and “neither showed an increased risk of infection from tap water. In fact, some cultures from allegedly sterile water bottles grew pathogenic bacteria, while no patient complications were reported in either study.” Current guidelines “recommend sterile water for procedures involving mucosal penetration but acknowledge low-quality supporting evidence.” However, they pointed out that “these recommendations are based on outdated studies, some unrelated to GI endoscopy.” Furthermore, the “review estimates that the production and transportation of sterile water bottles contributes over 6,000 metric tons of emissions per year from US endoscopy units alone.” The review was published in Gastro Hep Advances.
“With a conservative estimate of using half of a 1-L sterile bottle for irrigation per endoscopy, 22 million yearly endoscopies in the US could result in an additional 6000 tons of eCO2.”
Economic Costs:
“A 1-L bottle of sterile water costs $3–$10. For an endoscopy unit performing 30 procedures daily and a conservative estimate of half a water bottle per case, the average monthly direct costs could be $1000–$3000”
Discussion:
“There is no direct supporting evidence for using sterile water during endoscopy…a Cochrane review show no difference in infection risk when using tap or sterile water to irrigate wounds…Similarly, there is no benefit in using sterile water for enteral feeds in immunosuppressed patients, and tap water enemas are routinely acceptable for colon cleansing before sigmoidoscopies in all patients, irrespective of immune status.
My take: Plastic water bottles in endoscopy centers contribute to health-care waste, climate change and increased costs.
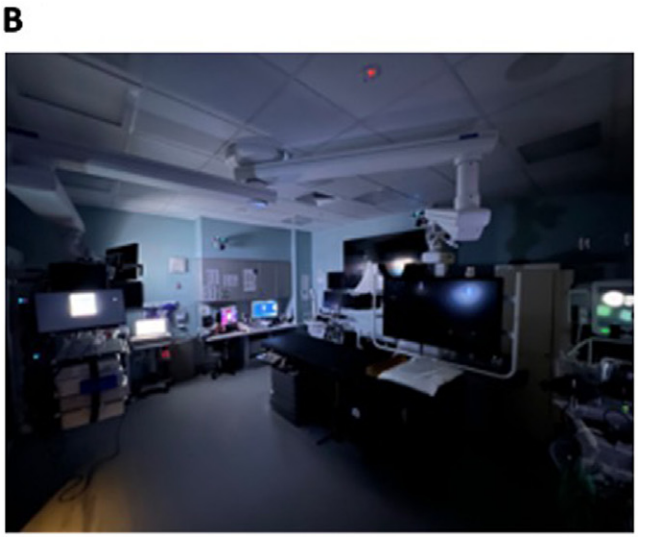
Background: “Unlike diagnostic radiology, GI endoscopy requires the concerted efforts of a proceduralist, anesthesiologist, nurse, and technician. Moreover, several of these individuals are often performing tasks that do not involve looking at a monitor. The advent of laparoscopic surgery presented surgeons with similar lighting challenges. In response to this problem, some operating rooms have been equipped with green lights to achieve high contrast and low glare on monitors while still allowing for the safe and efficient practice of other tasks in the operating room. The choice of green light is based on the fact that the human eye is most sensitive to light with a wavelength around 555 nm, in the green portion of the visible spectrum. This wavelength provides optimal contrast and sharpness under low-light conditions.”
Methods: The authors “conducted a single-center cross-over study comparing image classification on video monitors and the performance of multiple nonmonitored based physical tasks in the endoscopy suite using green light and dim light.”
Key findings:
Performance of physical tasks was significantly faster with green light, including endoscopy setup (43.1 vs. 62.1 s), biopsy sample time (35.8 s vs. 80.1 s), and feeding wire (34.3 vs. 99.1 s)
There was no difference in polyp detection rate under the 2 light conditions. However, color detection of anesthesia medication tapes and endoscopic tools was better with dim light.
Eye strain score was significantly better with green light compared with dim light (10.3 vs. 4.1)
My take: Use of green light in endoscopy suites is likely beneficial particularly in more technically-demanding procedures. It makes common tasks easier/quicker and with less eye strain.
(A) Endoscopy suite under green light. (B) Endoscopy suite under low light.
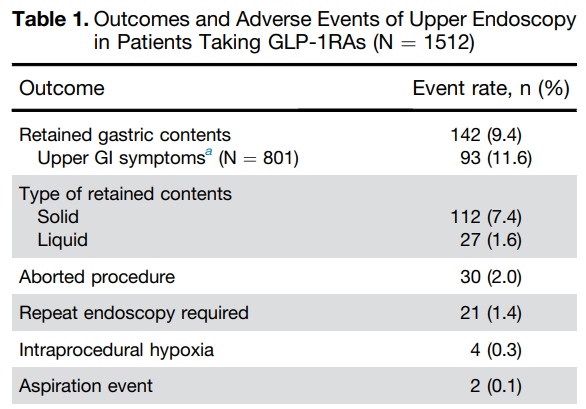
This is one of three articles discussing the issue of GLP-1RAs and potential complications with upper endoscopy. Faccisourruso et al performed a meta-analysis that included 13 studies (of 177 studies) involving a total of 84,065 patients.
Rates of aborted and repeated procedures were higher in the GLP-1RA user group. The absolute risk of aborted procedure was 1% in GLP-1RA users compared to 0.3% in non-users. The absolute risk of a repeated procedure was 2% vs 1% respectively.
No significant differences were found in AE and aspiration rates between the 2 groups (OR, 4.04 and OR, 1.75 respectively). The absolute risk of aspiration was 0.3% in GLP1-RA users compared to 0.2% in non-GLP1-RA group
Adverse events were higher in GLP-1RA users (0.3%) compared to non-users (0.1%)
In their discussion, the authors note that an “individualized approach based on the indication of GLP-1RA use (withholding the drug in patients with diabetes could lead to more harm)…a potential stragegy could be to place patients on a liquid diet the day before endoscopy, thus prolonging the duration of fasting for solid for at least 12 hours.”
My take: The totality of these studies confirms the increased risk of retained gastric contents in patients receiving GLP-1RAs. This in turn increases the need to abort/reschedule cases and may result in very a low increased risk of aspiration. To mitigate this risk, it may be sufficient to implement a liquid diet the day before endoscopy (avoiding solid foods for at least 12 hours prior to endoscopy). This is in agreement with the recent AGA Rapid Clinical Practice Update (see post below).
“Like millions of others, I was caught between what the food industry has done to make the American diet unhealthy and addictive and what my metabolism could accommodate.
We may now be at the brink of reclaiming our health. New and highly effective anti-obesity medications known as GLP-1s have revolutionized our understanding of weight loss and of obesity itself. These drugs alone are not a panacea for the obesity crisis that has engulfed the nation, and we should not mistake them for one. But their effectiveness underscores the fact that being overweight or obese was never the result of a lack of willpower…
GLP-1s are revolutionary drugs that can drastically reduce caloric intake and improve health in a way I didn’t expect I would ever see. Now we need to complete that revolution by taking on the food industry and its engineered foods that are contributing to some of the most harmful health issues America faces today.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
“GLP-1 RAs (eg, semaglutide, tirzepatide, exenatide, liraglutide, albiglutide, dulaglutide, and lixisneatide) mimic incretins, which are hormones released after eating that prompt glucose-dependent insulin release from the pancreatic islets, stimulate satiety centers, inhibit glucagon release, and result in diminished gastric emptying.”
Because GLP-1 RAs diminish gastric emptying, they can increase the risk of residual gastric contents prior to surgery and endoscopy.
AGA Recommendations:
“If patients taking GLP-1 RAs solely for weight loss can be identified beforehand, a dose of the medication could be withheld before endoscopy with likely little harm, although this should not be considered mandatory or evidence-based. Nevertheless, it is unclear if withholding the medication for only one dose would be reliably adequate for an individual’s gastric motility to return to normal. ..there is insufficient evidence to suggest this practice be performed for patients taking these medications to treat diabetes”
“Generally, in patients on GLP-1 RAs who have followed standard perioperative procedures (typically an 8-hour solid-food fast and a 2-hour liquid fast) and who do not have symptoms of nausea, vomiting, dyspepsia, or abdominal distention, we advise proceeding with upper and/or lower endoscopy.”
“When possible, placing patients on a liquid diet the day before sedated procedures may be a more acceptable strategy, in lieu of stopping GLP-1 RAs.”
My take: This guidance provides useful advice given the increasing use of GLP-1 RAs. If these medications are being used for obesity, holding a dose prior to endoscopy is a good idea.
Related article: S Sen et al. JAMA Surgery 2024; doi:10.1001/jamasurg.2024.0111.Glucagon-Like Peptide-1 Receptor Agonist Use and Residual Gastric Content Before AnesthesiaKey finding: Use of a GLP-1 RA was independently associated with increased residual gastric content (1.5 mL/kg of clear liquids on gastric ultrasonography) on preprocedural gastric ultrasonography: 56% (35 of 62) in patients with GLP-1 RA use (exposure group) compared with 19% (12 of 62) in patients who were not taking a GLP-1 RA drug (control group).
This is at the entrance to the Westside Reservoir Park. I had the chance to go there as part of a Westside Beltline Tour in Atlanta.This reservoir is as deep as the Statue of Liberty is tall and can hold 2.4 billion gallons of water for the city of Atlanta
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Thank you to those who have helped me this past year with this blog –colleagues, friends and family. Wishing all of you a good 2023. Here are some of my favorite posts from this past year:
In this retrospective study, “during a 20-month period until December 2021 using PPE and three different test approaches: no testing (n=4543), rapid antigen (RA) testing (n=682) and RT-PCR testing (n=10 465). In addition, 60 endoscopies were performed in patients with proven COVID-19. Not a single staff member became infected with SARS-CoV-2 during the 20 months analysed; vaccination rate of the team was 97%.”
The authors note that routine testing of clinical team was not performed; thus, they cannot exclude the possibility of asymptomatic infections.
My take (borrowed in part from authors): “PPE is highly effective for avoidance of SARS-CoV-2 transmission during upper or lower GI endoscopies.” Pre-op testing for COVID has many downsides: increased costs, delays in care, potential exacerbation of health disparities, and detrimental effects to endoscopy efficiency (especially with inconclusive results)
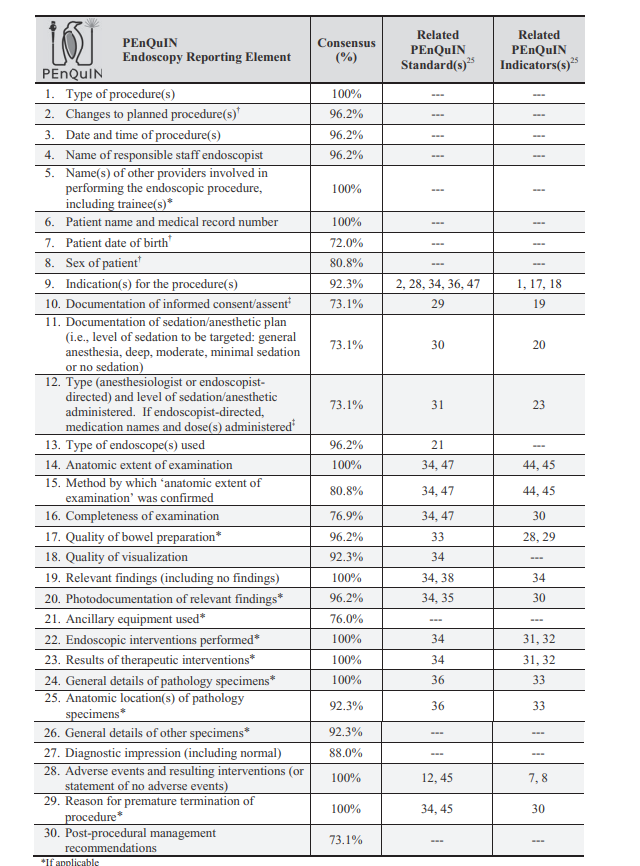
Several articles in a recent JPGN supplement issue describe the efforts to develop quality standards and indicators for pediatric endoscopy. All of these articles are open access.
My view: These detailed articles provide a good framework for improving pediatric endoscopy. After assuring that the facility and personnel are high quality, the pediatric endoscopist has the important responsibility of providing a high quality endoscopy. We need to strive to provide the best care for every single child entrusted in our care. In my view, the most important step is having an appropriate indication and despite guidelines, this remains highly subjective.
“AGA suggests against re-instituting routine pre-procedure testing prior to elective endoscopy. The downsides (delays in patient care, burden, inaccurate results) outweigh potential benefits. Infection and transmission of SARS-CoV2 from asymptomatic individuals is rare especially among vaccinated health care workers using personal protective equipment (PPE), even with the emergence of the Delta variant.”
“If PPE is available, AGA recommends using N95 masks” for both upper endoscopy and colonoscopy”
“AGA has now updated its July 2020 recommendations regarding pre-procedure testing. Based on the latest available data, routine COVID-19 testing prior to endoscopy is no longer needed to perform endoscopy safely.
Routine SARS-CoV-2 testing prior to endoscopy is no longer needed to perform endoscopy safely: Our systematic review found that there is little benefit in routine testing, given very low rates of infection (i.e. asymptomatic prevalence and transmission) during endoscopy to both patients and staff (0-0.5% across representative studies), with potential significant burden, including delays in care, impact of cancer burden, cost, health disparities and reduced endoscopy efficiency. Previously identified benefits of testing, including informed rationing of personal protective equipment (PPE) and patient and staff reassurance, have less relevance given adequate supply of PPE and reduced anxiety in later stages of the pandemic.
Vaccination status should not dictate decision-making for implementing pre-procedure SARS-CoV-2 testing: The studies included in our review were conducted prior to vaccination and show minimal benefit of testing as outlined above. While indirect data show that vaccination reduces that risk even further, the available evidence supports eliminating pre-procedure testing regardless of vaccination status of patients.
All patients should receive symptom screening prior to endoscopy: Centers should continue to implement universal screening of patients for COVID-19 symptoms, using a screening checklist, and follow universal precautions, including physical distancing, masks and hand hygiene in the endoscopy unit. For patients who have a positive symptom screen, pre-procedure testing can then be utilized for further triage.
For centers that value the small benefits (patient and staff reassurance or anxiety) over the downsides (delays care, potential exacerbation of health disparities, endoscopy efficiency, downstream consequences of false negatives and false positives), pre-procedure testing with rapid PCR tests can be considered: Rapid RT-PCR tests that can be performed on the day of endoscopy are preferable as they pose less burden to patients. In the pre-procedure setting, there is limited utility of rapid isothermal tests or antigen tests. There is no role for antibody tests in this context.”
These recommendations are only applicable IF:
My take: This is great news for our patients and hopefully will be widely adopted.