Methods: From May 2020 to May 2022, the authors performed a series of cross-sectional online surveys among a representative sample of adults ≥ 18 years old in the US (n=160,154). We administered Rome IV gastroduodenal and bowel DGBI questionnaires.
Key findings:
During the COVID-19 pandemic, the prevalence of irritable bowel syndrome (IBS) increased from 6.1% [May 2020] to 11.0% [May 2022]
In addition, the prevalence of chronic idiopathic constipation (CIC) increased mildly from 6.0% [May 2020] to 6.4% [May 2022]
No changes in prevalence were seen for the other examined gastroduodenal and bowel disorders of gut-brain interaction (DGBI)
My take: This study identified increases in the prevalence of IBS during COVID. Increases in IBS following other enteric infections (eg. norovirus, shigella, campylobacter) has been shown previously as well.
I was a little disappointed (aka first world problem) that this commentary appeared in the February print edition of The Journal of Pediatrics about 4 months after the publication of the analyzed study. This blog commented on this study in October: Disparities Are Abundant in Pediatrics -4 Studies on IBD, SUID, Specialty Referrals and in the NICU re: J Smith et al. J Pediatr 2023; 260: 113522.
“In this issue of The Journal, Smith et al report the results of an historical cohort analysis of 519 children and adolescents with newly diagnosed IBD (2013-2020)… Smith et al ask the question of whether the greater rate of complicated disease in Black patients is related more to delayed diagnosis or access to therapy rather than inherent race-based differences in response to treatment.”
Key points:
“In this study, Smith et al importantly identified no difference in initiating standard medical therapies based on race. Specifically, they report no difference in initial corticosteroid usage, time to initiation of maintenance therapy, or time to initiate antitumor necrosis factor therapy. In patients receiving biologics, both Black and White patients received similar loading doses and frequency of therapeutic drug monitoring.”
“Despite comparable disease presentation and approach to medical therapy in this study cohort,Black patients strikingly remained only one-half as likely to reach corticosteroid-free remission at 12 months compared with White patients (OR 0.52, 95% CI 0.3-0.9).”
” Black patients were less likely to be seen in gastroenterology specialty clinic for follow-up, more likely to present to the emergency department, and more likely to be hospitalized.”
“This study described poorer outcomes in Black patients despite similar treatments. However, the authors fail to arrive at a definitive answer as to why this is the case.”
My take: Black patients, even when offered similar IBD treatment, clearly experience inferior outcomes. While access and social determinants of health are important, there may be biological/phenotypic factors (eg. more aggressive disease) that are involved as well. More studies are needed. This editorial is a helpful review -the timing of the editorial in the print edition many months later, though, is a head-scratcher.
Unrelated topic: CDC COVID-19 Recommendation
The Centers for Disease Control and Prevention announced new isolation guidance for Covid-19 this week. At the start of the pandemic, people were recommended to stay home for 10 days after testing positive. At the height of the Omicron wave, that was revised to 5 days. This week, isolation time was revised to 24 hours without a fever and symptoms improving, which is similar to the recommendations for other illnesses.
Methods: To examine cognitive slowing, patients with post-COVID-19 conditions (PCC) completed two short web-based cognitive tasks, Simple Reaction Time (SRT) and Number Vigilance Test (NVT). 270 patients diagnosed with PCC at two different clinics in UK and Germany were compared to two control groups: individuals who contracted COVID-19 before but did not experience PCC after recovery. For the SRT, participants were required to press the spacebar when a large red circle appeared in the center of the screen.
.**The simple reaction time task and the number vigilance task can be tried online at [https://octalportal.com/pcc]..
Key finding:
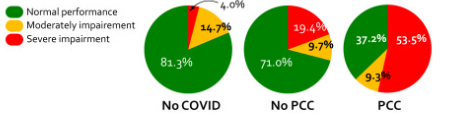
There was pronounced cognitive slowing in patients with PCC, which distinguished them from age-matched healthy individuals who previously had symptomatic COVID-19 but did not manifest PCC. Cognitive slowing was evident even on a 30-s task measuring simple reaction time (SRT), with patients with PCC responding to stimuli ∼3 standard deviations slower than healthy controls. 53.5% of patients with PCC’s response speed was slower than 2 standard deviations from the control mean, indicating a high prevalence of cognitive slowing in PCC.
Comorbidities such as fatigue, depression, anxiety, sleep disturbance, and post-traumatic stress disorder did not account for the extent of cognitive slowing in patients with PCC.
Cognitive slowing on the SRT was highly correlated with the poor performance of patients with PCC on the NVT measure of sustained attention.
Results of simple reaction time
My take (borrowed from authors): Using a 30-s web-based, self-administered psychomotor task, cognitive slowing in PCC can be reliably and easily measured as part of diagnostic work-up, and has potential to be a biomarker to track the progress of rehabilitation of PCC.
**The simple reaction time task and the number vigilance task can be tried online at [https://octalportal.com/pcc].
It used to be fairly easy to dismiss Florida’s surgeon general, Dr. Joseph A. Ladapo, as a clownish anti-vaccine quackposing a danger mostly to residents of his home state…Ladapo has moved from promoting useless treatments for COVID-19, such as the drugs hydroxychloroquine and ivermectin, to waging an ever-expanding fact-free campaign against the leading COVID vaccines…
That brings us to Ladapo’s latest adventure in medical quackery, his claim that no one should take the mRNA vaccines….Ladapo’s advice is based on what he says is research that the Pfizer and Moderna mRNA COVID vaccines contain fragments of DNA that are injected into human cells, which they can contaminate and turn into cancer cells…
The human cell has a panoply of mechanisms to destroy foreign DNA. Even if the fragments managed to penetrate the cell nucleus, which can’t happen, they would have to cut up the existing DNA, which would require a mechanism the fragments don’t have.
“So the chancethatDNA could affect yourDNA is zero,” Offit said..
Ladapo’s words and actions have surely contributed to his state’s pathetic performance in getting its citizens vaccinated against COVID. With 11.6% of its population fully vaccinated with a booster as of last May, Florida had a rate among the lowest in the nation. (California’s rate was 20.6%.) Among those 65 and older — purportedly the population that Florida strives to protect — only 31.2% were fully vaccinated. (California: 48.3%.)
Florida’s death rate from COVID of 375 per 100,000 people is among the worst in the country. (California: 283.) You can ignore the defense that the difference is due to Florida’s relatively older population; states with even older median ages have done much better: Vermont (170), New Hampshire (245) and Maine (252). The difference is the indifference of Ladapo and DeSantis to their own residents’ health.
Hydroxychloroquine (HCQ) was used off-label for COVID-19 during the first wave despite the absence of evidence documenting its clinical benefits. A recent study has estimated that it resulted in an increase death rate of 11%. ”The number of hydroxychloroquine related deaths in hospitalized patients is estimated at 16,990 in six countries.” Ref: Open Access! A Pradelle et al. Biomedicine & Pharmacotherapy 2024; 171: 116055. Deaths induced by compassionate use of hydroxychloroquine during the first COVID-19 wave: an estimate
Florida’s surgeon general on Wednesday called for a halt to the use of Covid vaccines, citing widely debunked concerns that contaminants in the vaccine can permanently integrate into human DNA.
Dr. Ladapo’s latest contention is “very irresponsible,” said John Wherry, a vaccine expert and director of the Institute for Immunology at the University of Pennsylvania. “He has, however, demonstrated a tenuous grasp of science and medicine in general over the course of the pandemic so this is not surprising,” Dr. Wherry said….
For Dr. Ladapo’s claim to be true, humans would need to have an enzyme that can incorporate foreign DNA into their genomes. “We don’t have one,” said Dr. Eric Rubin, a member of the F.D.A.’s vaccine advisory committee and the editor in chief of the New England Journal of Medicine.
My take: The first article estimates the number of deaths due to the bad advice of using hydroxychloroquine. Perhaps in a few years, researchers will be able to calculate the number of deaths and hospitalizations that occur due to the bad advice of Florida’s surgeon general.
Methods: This population study assessed all confirmed cases of BA, from January 2020 to December 2021 across the 3 UK pediatric liver centers originating from England and Wales. Data was then compared to the incidence of confirmed BA cases from January to December 2017, 2018, and 2019.
Key findings -BA cases:
2017: 16
2018: 13
2019: 18
2020: 8
2021: 12
This difference was significant in a two-sided t test for 2020 (P = 0.035) but not for 2021 (P = 0.385)
The authors note that new BA diagnoses were reduce among Danish centers as well. In their discussion, the authors discuss the possibility of missed diagnosis versus an actual drop in BA cases. The later is intriguing due to concerns that perinatal infections could trigger BA.
My take: This study provides a piece of a puzzle regarding the etiology of BA, indicating a good likelihood of environmental/infectious etiologies as a trigger.
The Florida Surgeon General’s recommendation that young men shouldn’t get the COVID-19 vaccine was made “despite the state having contradictory data,” according to the Tampa Bay Times.
In October, Florida Surgeon General Joseph Ladapo, MD, PhD, announced that young men shouldn’t get the COVID-19 vaccine, countering CDC guidance. His recommendation was based on an analysis that purported to show an increased risk of cardiac-related death for men ages 18 to 39.
However, draft versions of the analysis obtained by the Tampa Bay Times show that “catching COVID-19 could increase the chances of a cardiac-related death much more than getting the vaccine,” the article stated.
“That data was included in anearlier version of the state’s analysis but was missing from the final version compiled and posted online by the Florida Department of Health,” the Times reported. “Ladapo did not reference the contradictory data in a release posted by the state.”
My take: The approach taken by Florida’s “surgeon general” is one of making sure the facts don’t get in the way of a perfectly good narrative.
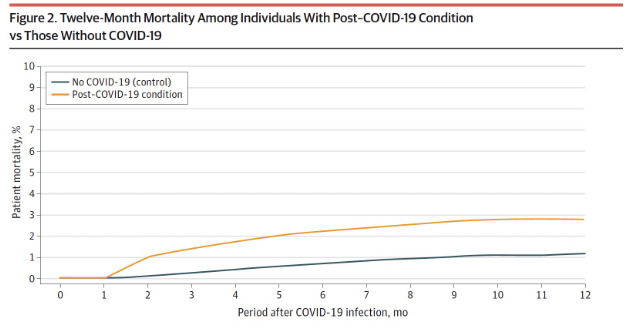
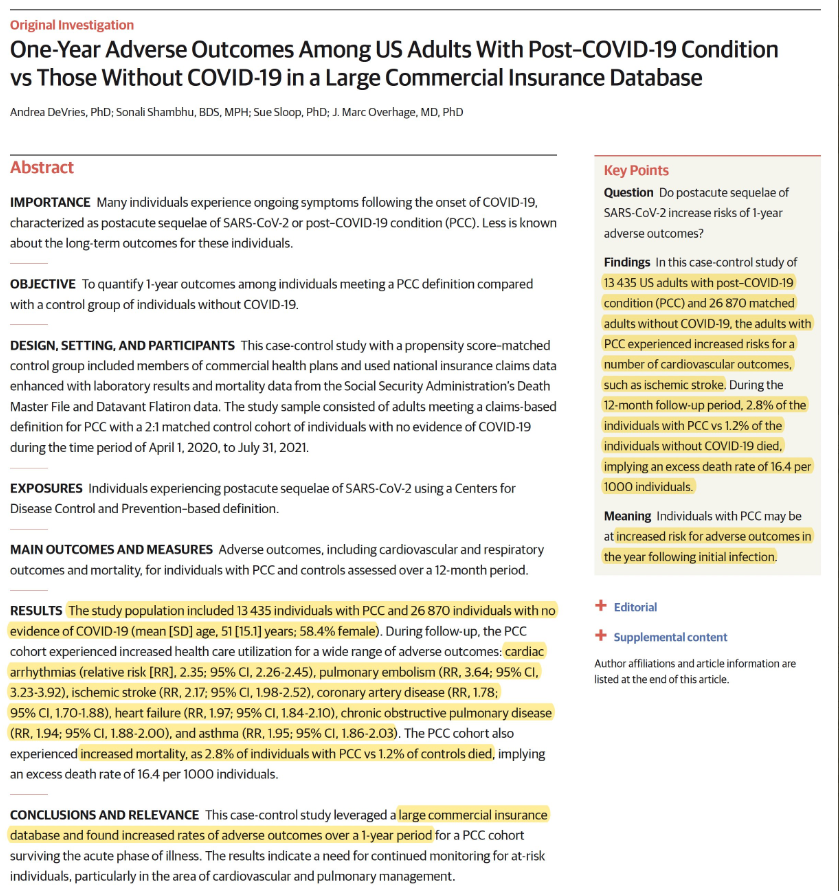
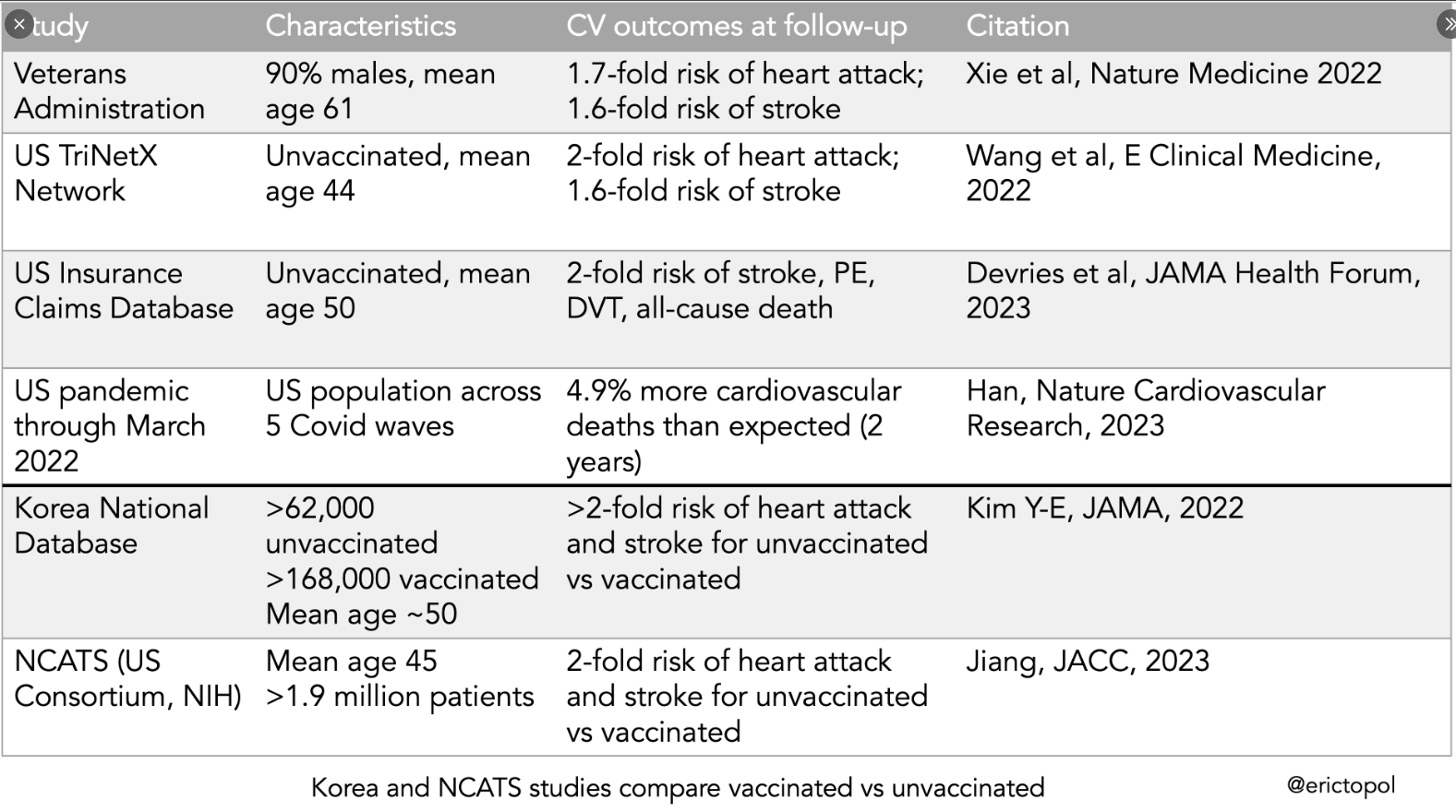
This case-control study leveraged a large commercial insurance database and found increased rates of adverse outcomes over a 1-year period for a post-COVID-19 cohort surviving the acute phase of illness. Methods: An index month was set by adding 30 days to the COVID-19 diagnosis date (this study looked at outcomes starting one month after diagnosis).
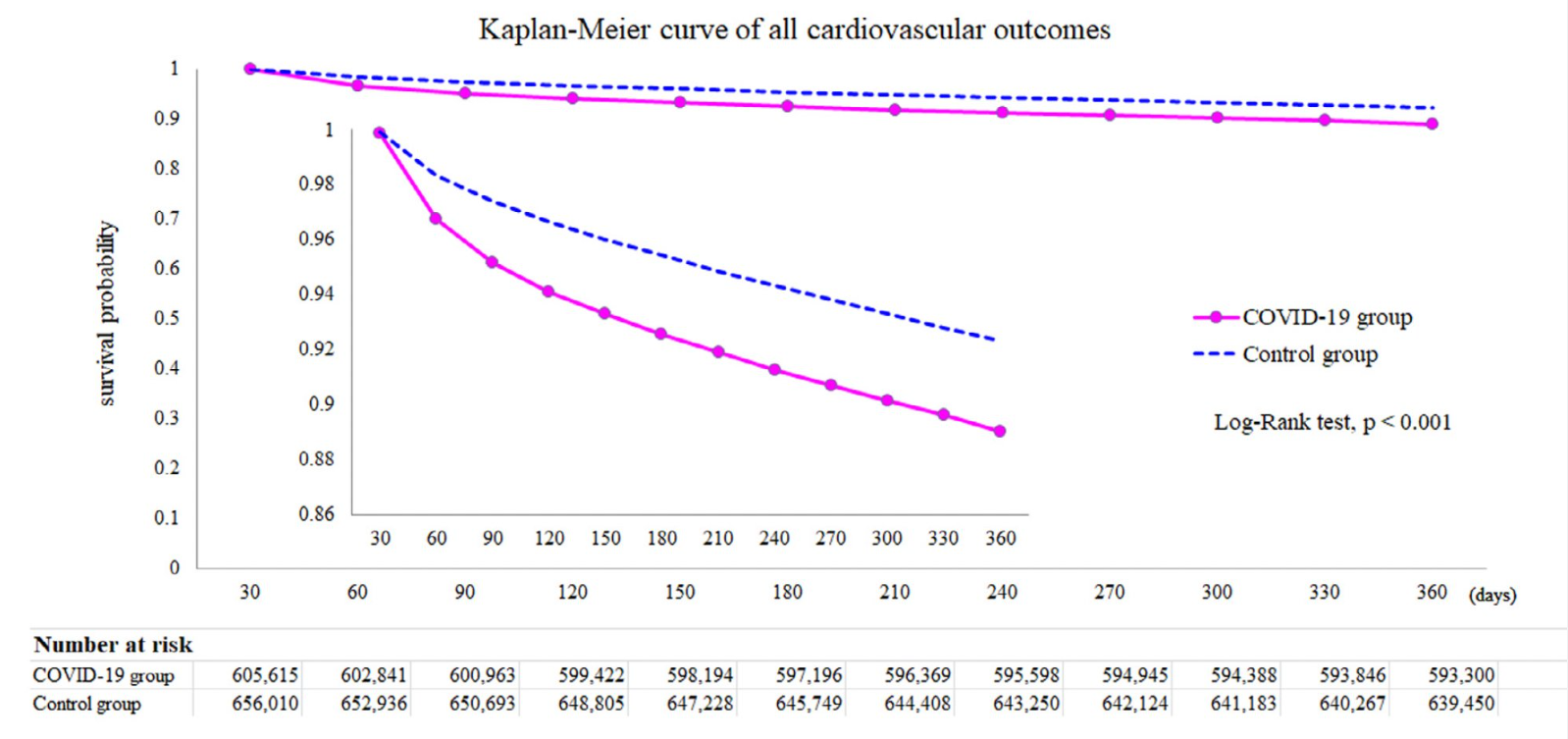
This study used the data from the US Collaborative Network in TriNetX. From a cohort of more than 42 million records between 1 January 2019 and 31 March 2022, a total of 4,131,717 participants who underwent SARS-CoV-2 testing were recruited.
My take: Many detractors of vaccination have focused on potential cardiac adverse events. These studies indicate that COVID vaccination provides protection against major cardiovascular outcomes
This article recommends medical schools stop participating in U.S. News & World Report’s (USNWR) ‘best medical school’ survey. I would advocate for eliminating USNWR’s reports more broadly including their ranking of hospitals and medical specialties.
The medical school rankings rely on the following:
Federal research dollars
Reputation – “assessed by a survey (with an abysmal response rate) of medical school deans, department chairs, and residency program directors”
Ratio of full-time faculty to students
Students’ median scores on the Medical College Admission Test and their undergraduate grade-point averages
Acceptance rate
Some excerpts:
“Yale and Harvard Law Schools recently announced they would no longer participate in U.S. News & World Report’s (USNWR) flawed ranking system, followed closely by additional schools. The nation’s medical schools need to follow their lead. Why? The USNWR ranking system is in direct opposition to medical schools’ goal of educating a well-trained, diverse, and culturally competent medical workforce..”
“It is hardly a secret among medical school deans that the USNWR rankings are based on data not directly related to educational process, quality, and outcomes. Nor can they trust the veracity of the data that are provided, given the recent scandals reported in other professional schools and colleges that manipulate the formula to their own advantage.”
“Comprehensive analyses of USNWR rankings have long demonstrated that the methodology is ill-conceived, that the response rate of those completing the questionnaires that feed into the ranking formula would not meet the standards of a peer-reviewed publication, and that the most important aspects of educational quality are largely ignored.”
“There is peer pressure to stay within the system and to compete for the top prize because it feels good to see your school on top, no matter how flawed the measuring stick.”
My take: It is difficult to measure quality. I do not trust USNWR’s rankings with regard to “best” medical school, “best” hospital or “best” subspecialty. I think medical care would be better off without these reports. Another option would be to focus on reporting hard data, rather than the current aggregate format. This data could include federal research dollars and reputational surveys; the latter would need to be transparent with regard to methodology.
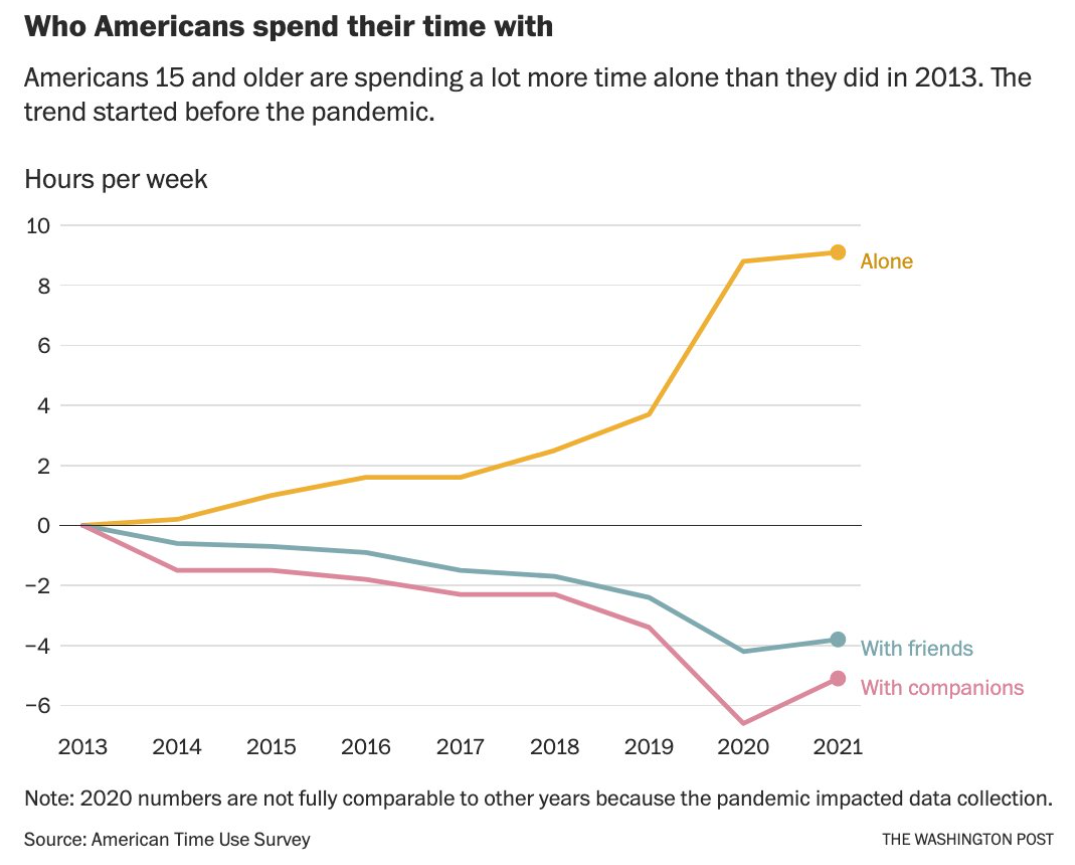
From TheWashington Post, 11/23/22. Opinion Americans are choosing to be alone. Here’s why we should reverse that. “Spending less time with friends is not a best practice by most standards, and it might contribute to other troubling social trends — isolation, worsening mental health (particularly among adolescents), rising aggressive behavior and violent crime. “
Methods: In this 5-year retrospective study, the authors identified 22 patients with NRCD; they were following a gluten-free diet for at least 12 months but had persistent symptoms and enteropathy (Marsh 3). Treatments for NRCD were either a GCED (n=13), budesonide (n=9) or both (n=4). Four patients were lost to follow-up and did not receive either treatment.
Key findings:
Thirteen were treated with the GCED for 3 months with 46% achieving both histological and symptomatic resolution
Nine patients were treated with budesonide (6–9 mg daily), with 89% achieving both symptomatic and histologic resolution after a median 3-month treatment course
67% of patients who responded to the GCED and 100% of patients who responded to budesonide remained in remission for at least 6 months following treatment transition back to exclusive GFD
My take: This important article shows that many patients thought to be receiving a GFD can respond to a more stringent approach. In addition, it offers an alternative strategy with budesonide which had a high response rate.
In patients believed to have celiac disease who have persistent or recurrent symptoms or signs, the initial diagnosis of celiac disease should be confirmed by review of prior diagnostic testing, including serologies, endoscopies, and histologic findings.
Best Practice Advice 2
In patients with confirmed celiac disease with persistent or recurrent symptoms or signs (nonresponsive celiac disease), ongoing gluten ingestion should be excluded as a cause of these symptoms with serologic testing, dietitian review, and detection of immunogenic peptides in stool or urine. Esophagogastroduodenoscopy with small bowel biopsies should be performed to look for villous atrophy. If villous atrophy persists or the initial diagnosis of celiac disease was not confirmed, consider other causes of villous atrophy, including common variable immunodeficiency, autoimmune enteropathy, tropical sprue, and medication-induced enteropathy.
Best Practice Advice 3
For patients with nonresponsive celiac disease, after exclusion of gluten ingestion, perform a systematic evaluation for other potential causes of symptoms, including functional bowel disorders, microscopic colitis, pancreatic insufficiency, inflammatory bowel disease, lactose or fructose intolerance, and small intestinal bacterial overgrowth.
Best Practice Advice 4
Use flow cytometry, immunohistochemistry, and T-cell receptor rearrangement studies to distinguish between subtypes of refractory celiac disease and to exclude enteropathy-associated T-cell lymphoma. Type 1 refractory celiac disease is characterized by a normal intraepithelial lymphocyte population and type 2 is defined by the presence of an aberrant, clonal intraepithelial lymphocyte population. Consultation with an expert hematopathologist is necessary to interpret these studies.
Best Practice Advice 5
Perform small bowel imaging with capsule endoscopy and computed tomography or magnetic resonance enterography to exclude enteropathy-associated T-cell lymphoma and ulcerative jejunoileitis at initial diagnosis of type 2 refractory celiac disease.
Best Practice Advice 6
Complete a detailed nutritional assessment with investigation of micronutrient and macronutrient deficiencies in patients diagnosed with refractory celiac disease. Check albumin as an independent prognostic factor.
Best Practice Advice 7
Correct deficiencies in macro- and micronutrients using oral supplements and/or enteral support. Consider parenteral nutrition for patients with severe malnutrition due to malabsorption.
Best Practice Advice 8
Corticosteroids, most commonly open-capsule budesonide or, if unavailable, prednisone, are the medication of choice and should be used as first-line therapy in either type 1 or type 2 refractory celiac disease.
Best Practice Advice 9
Patients with refractory celiac disease require regular follow-up by a multidisciplinary team, including gastroenterologists and dietitians, to assess clinical and histologic response to therapy. Identify local experts with expertise in celiac disease to assist with management.
Best Practice Advice 10
Patients with refractory celiac disease without response to steroids may benefit from referral to a center with expertise for management or evaluation for inclusion in clinical trials.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.