P Martin et al. Clin Gastroenterol Hepatol 2022; 20: 1766-1775. Open access! Treatment Algorithm for Managing Chronic Hepatitis B Virus Infection in the United States: 2021 Update
This article provides an updated treatment algorithm with many changes since 2015.
Key points:
New terminology. The authors provide updated terminology. The term ‘immune tolerant’ is losing favor. “There is also evidence that during the immune tolerant phase virologic events occur, such as integration of viral DNA into the host genome, which may help set the stage for the subsequent development of HCC.” As such, the new terminology focuses on “describing the 2 main characteristics of chronicity, infection alone and infection with evidence of ongoing hepatic inflammation (ie, hepatitis).” (See below)
TAF preferred over TDF. “The 4 first-line therapies available for managing CHB infection in the United States are peginterferon alfa-2a, entecavir (ETV), tenofovir disoproxil fumarate (TDF), and tenofovir alafenamide (TAF)….It is the opinion of most—but not all—members of the panel that when antiviral therapy is contemplated, TAF is preferred over TDF because of the lower risks of renal or bone side effects and higher likelihood of ALT normalization through 48 weeks.” For decompensated cirrhosis, TAF and peginterferon are NOT recommended.
Long term treatment is the rule (not the exception). “HBeAg-positive patients with evidence of less extensive fibrosis (<F3) should be treated long-term, even after HBeAg seroconversion and virologic suppression because of the risks of virologic relapse55 and ALT flares, except when treatment is initiated solely for the purpose of prevention of vertical transmission…For HBeAg-negative patients without HBsAg seroconversion, the panel does not recommend stopping treatment.”
Monitoring. “Primary nonresponse to ETV, TDF, or TAF is rare; therefore, any patients who are not responsive to these agents after 12 to 24 weeks should be evaluated for compliance.”
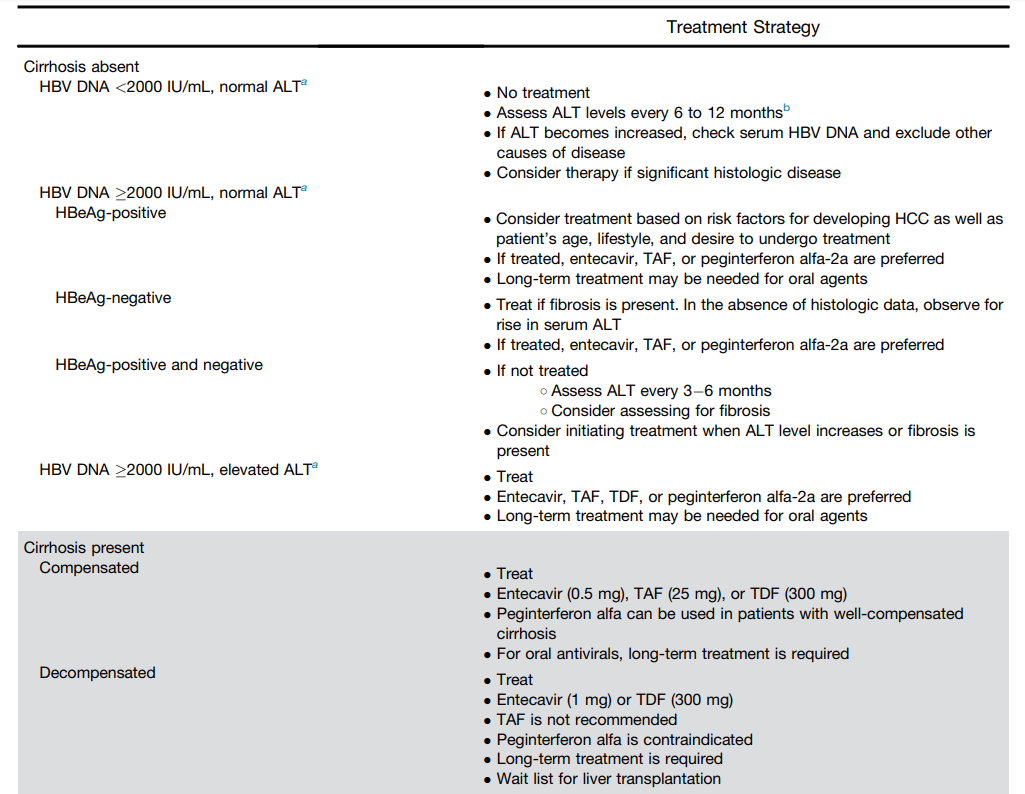
Table 1 (see below) summarizes treatment recommendations. In almost all patients with HBV, if there is elevated ALT, treatment is recommended.
Terminology:

Table for Treatment Recommendations:
for treatment in the setting of HIV coinfection
My take: Forget about “immunotolerant” HBV. Until better treatments emerge, patients with HBV and elevated liver enzymes are likely to need long-treatment if using TAF, TDF or entecavir.
Related blog posts:
- Big Advance for Hepatitis B, Plus One | gutsandgrowth
- When can you safely stop nucleos(t)ides for hepatitis B?
- Is Tenofovir the Best Medication for Hepatitis B Infections?
- Liver Shorts: PFIC/FIC1, Best Tenofovir, Ascites Practice Guidance
- New Hepatitis B Treatment Guidelines (2015)
- Why Fewer Children Have Immune-Tolerant Hepatitis B Infection Than Previously
- Preventing Neonatal Hepatitis B Transmission with Tenofovir | gutsandgrowth
- Hepatitis B: Natural History and Difficulty Treating Immunotolerant Children | gutsandgrowth