A recent blog post summarized the recent Rome V recommendations which include useful tips for the diagnosis and management of Cannabinoid Hyperemesis Syndrome (Reference article: R Rosen et al. Gastroenterol 2026; 170: 1347-1366. Open Access! Rome V Pediatric Upper Gastrointestinal Disorders of Gut-Brain Interaction).
A practice management article by Nguyen et al (The Journal of Pediatrics, 2026; 291: 114966. Management of Cannabinoid Hyperemesis Syndrome in Adolescents and Young Adults) provides a lot of granular detail on how to improve outcomes.
Clinical manifestations:
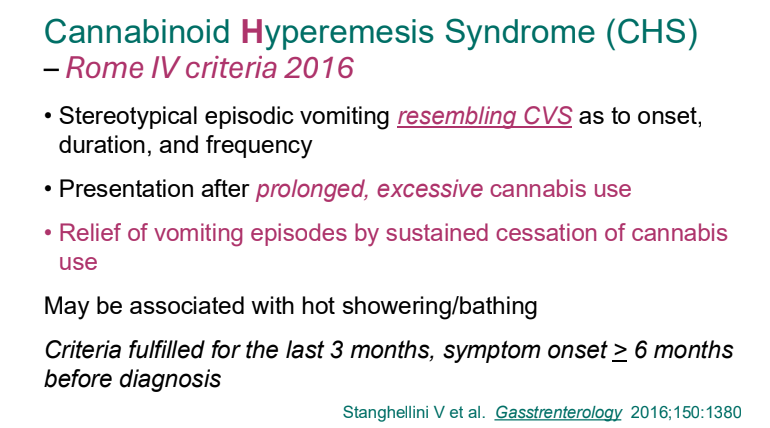
- “Recurrent vomiting that is not attributable to another disorder and in the context of cannabis use should raise concerns for cannabinoid hyperemesis syndrome (CHS). CHS typically presents with three phases. The prodromal phase is characterized by abdominal discomfort and early morning, episodic nausea on at least 1 day per week. This prodrome
may precede acute vomiting by months or years. The emetogenic phase is characterized by sudden-onset, severe vomiting and abdominal pain episodes. Symptoms start within
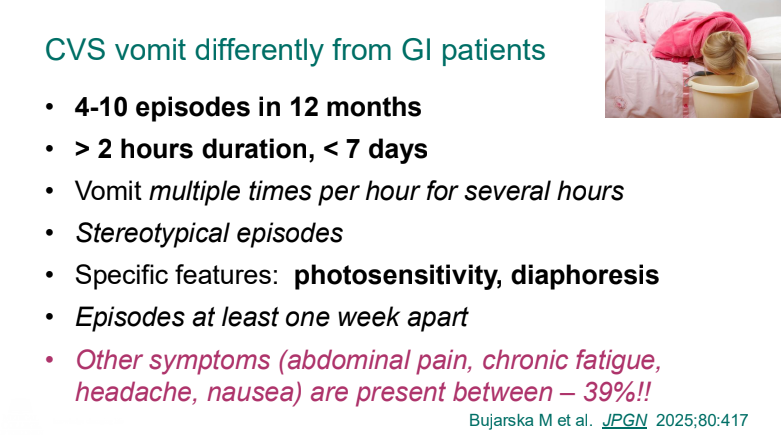
24 hours of last cannabis use, last typically for 24-48 hours, and may persist for up to 7-10 days. Abdominal pain is usually described as cramping in nature, radiating diffusely from
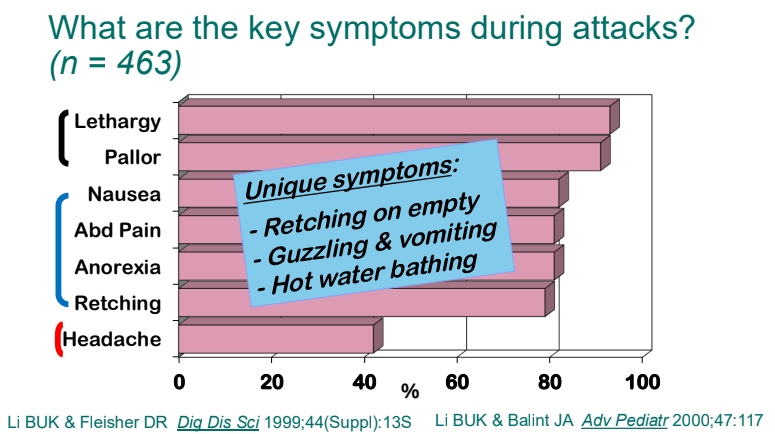
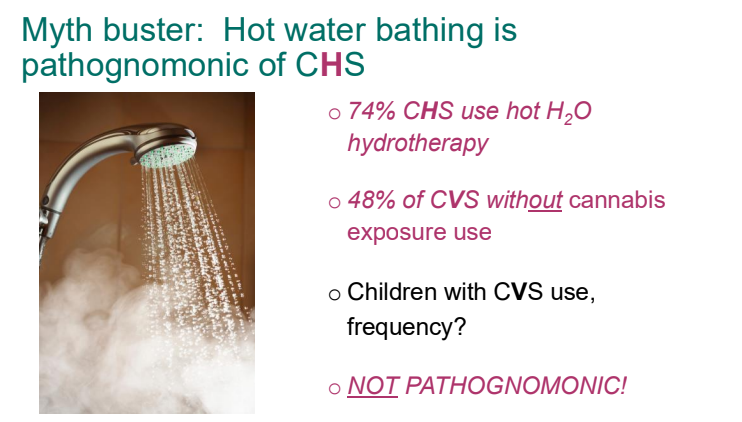
the epigastrium or umbilicus. Patients often report symptom improvement with hot showers or baths. Acute nausea and vomiting gradually abate if patients abstain from cannabis, allowing transition from the acute emetogenic phase to the recovery phase and normalization of eating patterns. Symptoms typically recur with re-exposure to
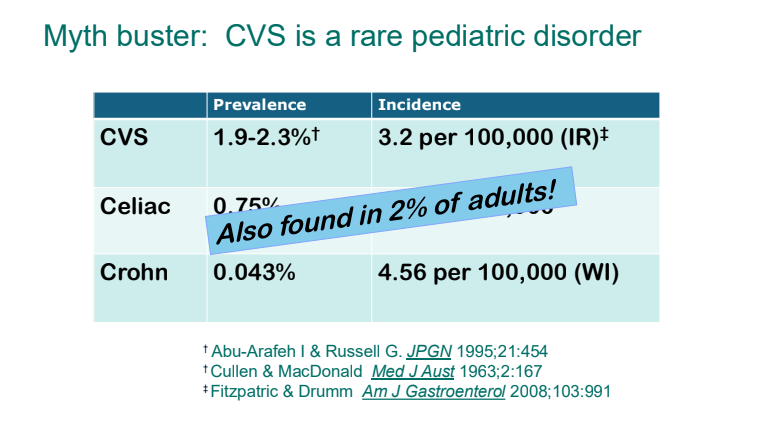
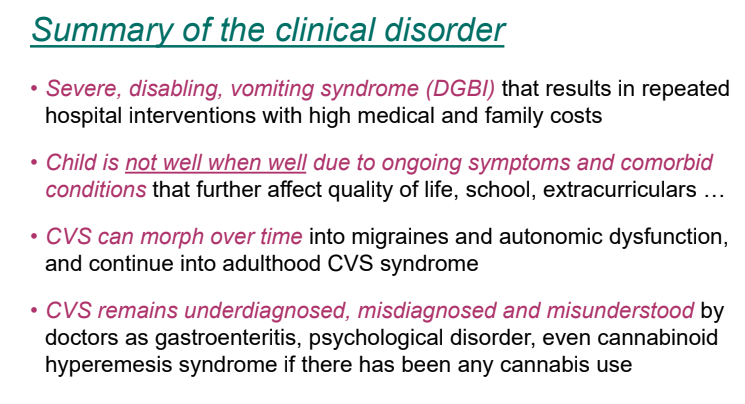
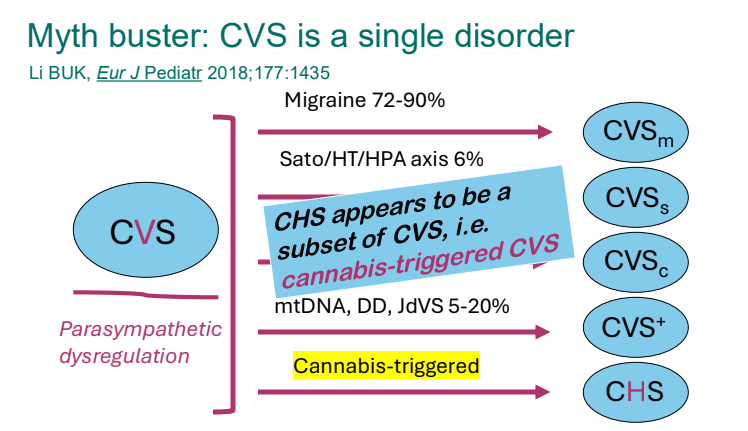
cannabis.” - “CHS is a separate disorder from CVS. It is critical that medical providers avoid providing CHS and CVS as interchangeable diagnoses to patients and families. Inconsistent
diagnoses may erode families’ trust in the health care system by giving the impression that providers have not yet settled on an etiology. Furthermore, patients experiencing CHS
who learn more about CVS outside the formal medical setting may gather that prophylactic medications are the mainstay of episode prevention, rather than cannabis cessation and abstinence.”
Evaluation:
- “Bloodwork should include a comprehensive metabolic panel with liver function testing, complete blood count with differential, lipase, urinalysis, and a qualitative urine pregnancy test in a person capable of pregnancy.”
- “An electrocardiogram is indicated if a patient has received multiple antiemetics, has an electrolyte abnormality, or is severely malnourished.”
- “Abdominal imaging is most helpful to evaluate for suspected structural pathology.”
- “A quantitative urine THC level may be helpful for longterm management of adolescents and young adults…A small study in adolescent patients suggests that urine THC levels >100 ng/mL are associated with cannabinoid hyperemesis syndrome….The test may be clinically useful to demonstrate significant marijuana exposure for patients who do not think their use is sufficient to cause their symptoms”
Management:
- “Inpatient management can be conceptualized as having two phases. During the first 24 hours, patients require aggressive, proactive management. The goal isto break the vomiting
cycle.” - “Our group’s practice is to select a single antiemetic with evidence in CHS treatment and to schedule this medication at the lowest therapeutic dose for vomiting relief at an interval that prevents recurrence of vomiting. An additional medication may be used as needed for breakthrough symptoms.”
- “We typically use olanzapine or haloperidol as the initial agent. We recommend avoiding the use of multiple unscheduled antiemetics ordered “as needed” for nausea and vomiting. This approach risks drug interactions and QTc prolongation.” Typical antiemetics like ondansetron and prochloroperazine are usually ineffective for CHS.
- “Regular application of capsaicin cream during the acute phase can decrease the need for oral medications by reducing or eliminating nausea and modestly reducing abdominal pain…We use capsaicin 0.1% cream in our clinical setting.”
- “In the second phase of treatment, as the emetogenic phase abates and the patient can sustain oral nutrition, providers should focus on transitioning to a safe outpatient antiemetic
plan.” - “Patients with pre-existing inherited or acquired long QTc should be treated with caution…When a prolonged QTc is identified, providers should consider using topical capsaicin and medications less likely to increase QTc, including lorazepam and aprepitant.”
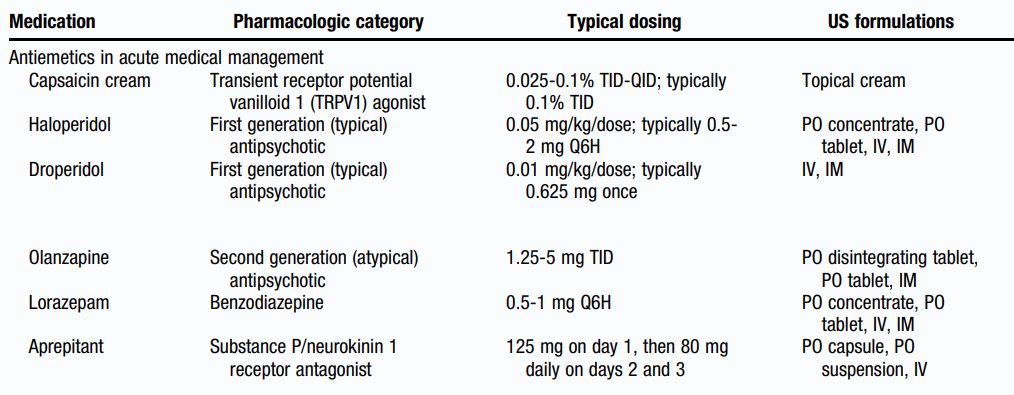
**The use of lorazepam and aprepitant have only been report in case studies for CHS.
**Aprepitant can be administered intravenously as a one-time dose.
**Benzodiazepines should be limited to first 24-48 hours due to risk of addcition.
Malnutrition Often Associated with Chronic Cannabis Use:
- Despite its perception as causing the ‘munchies,’ “chronic cannabis use is an underrecognized cause of weight loss and malnutrition. The insidious morning nausea and
abdominal pain of the CHS prodrome can contribute to gradual weight loss, and a rapid weight drop may occur with vomiting episodes.” - “Potential medical complications of significant malnutrition include bradycardia, hypotension, hypothermia, orthostatic lightheadedness or presyncopal/syncopal episodes, cold intolerance, fatigue, worsening mood and anxiety, and change in menses…increases risks of superior mesenteric artery syndrome and the refeeding syndrome.”
Outpatient Management of CHS:
- “Long-term management of CHS prioritizes cannabis abstinence, reestablishment of normal eating, and return to full daily function, including consistent participation in school
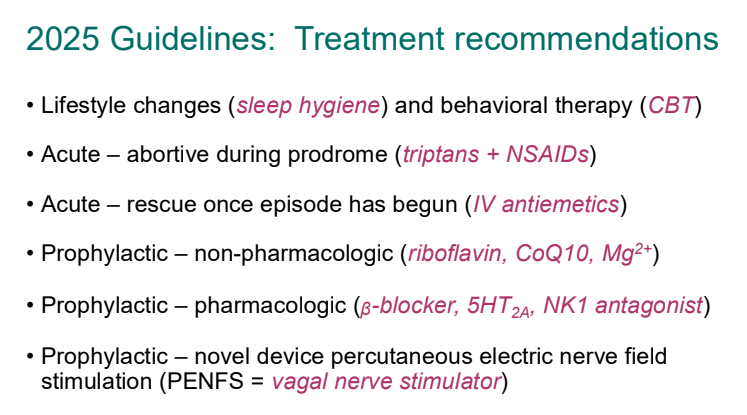
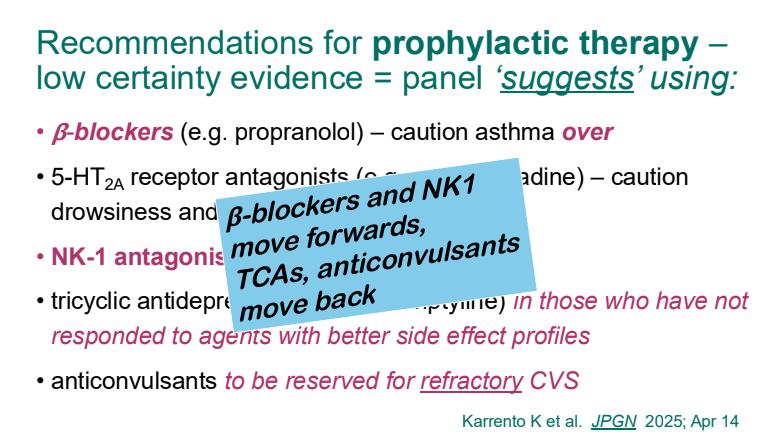
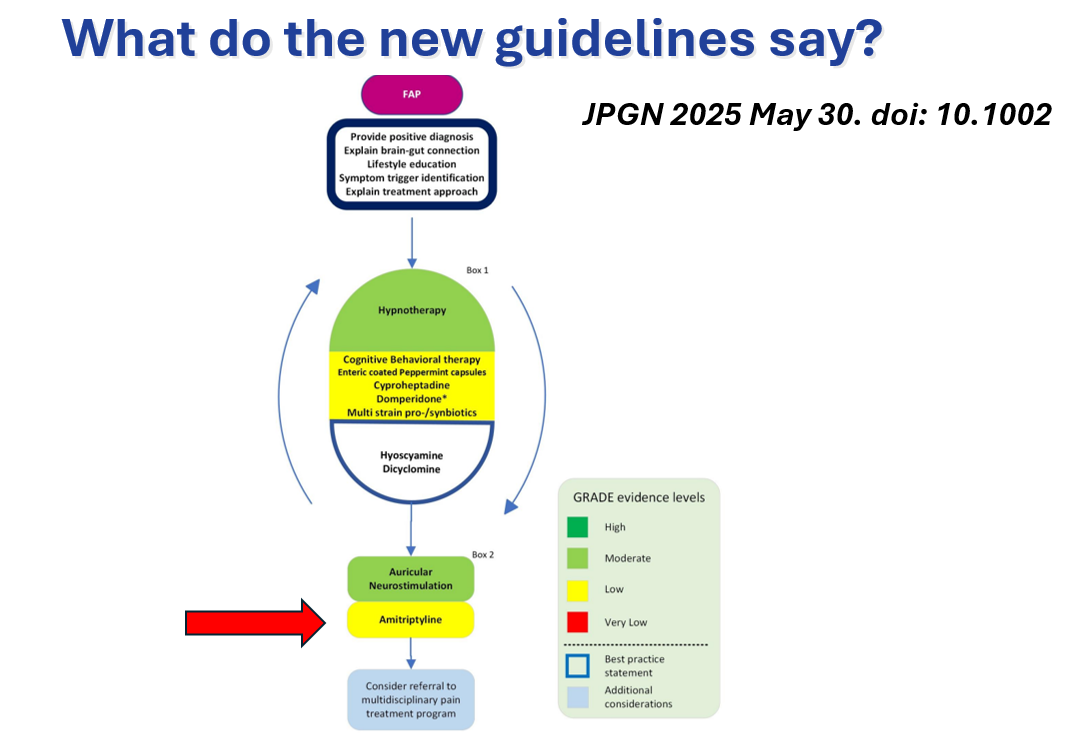
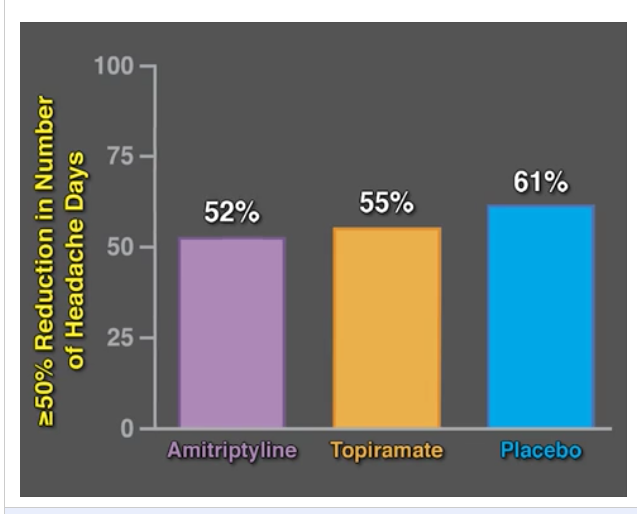
and/or employment.” - “Indications for CHS prophylactic medication are extrapolated from existing literature in
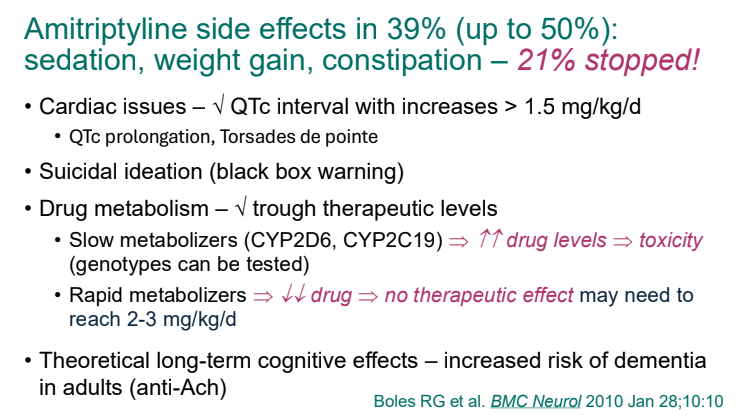
adults with CVS. Prophylaxis should be considered if exacerbations occur more frequently than once a month and last for over 2 days in an adolescent…Amitriptyline, a tricyclic antidepressant, is the first line agent for CHS prophylaxis…Nortriptyline, which is less sedating than amitriptyline, has also shown success in children and adults with CVS.” The authors discussed typical dosing of amitriptyline and nortriptyline (starting at 10-25 mg and titrating up to 1 to 1.5 mg/kg at bedtime [max 75 mg to 100 m]) - “We continue the tricyclic antidepressant until hyperemesis exacerbations have been suppressed and the patient has maintained cannabis abstinence for 6-12 months, then slowly taper prophylaxis.”
- “CHS is definitively treated with complete cessation and long-term abstinence from marijuana use for weeks to months. Focused treatment of concurrent cannabis use disorder is critical to recovery. We note that patients who intend to abstain from cannabis often struggle for 2-4 weeks after cessation due to withdrawal symptoms.”
My take: This article offers a lot of practical advice for CHS.
Related blog posts:
- AGA Practice Update: Cannabinoid Hyperemesis
- How to Distinguish Cyclic Vomiting Syndrome and Cannabis Hyperemesis Syndrome
- Capsaicin for Cannaboid Hyperemesis Syndrome
- 2025 Pediatric Cyclic Vomiting Syndrome Guidelines
- Dr. B Li: Cyclic Vomiting Syndrome 2025
- Cannabis Toxic Effects
- Does Stopping Cannabis Improve Cyclic Vomiting Syndrome?
- Getting In the Shower for Emetic Symptoms
- Aprepitant for CVS
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.