Ironwood Pharmaceutical Press Releasse, 5/27/26: FDA Approves Use of LINZESS® (linaclotide) in Pediatric Patients Two Years of Age and Older with Functional Constipation (FC)
An excerpt:
Expanded indication extends availability to children ages 2-5 with FC; previously approved in pediatric patients 6 years of age and older –
– LINZESS remains the first-and-only FDA-approved prescription therapy for pediatric FC…
Parents can mix the contents of the LINZESS capsule with applesauce or water, providing flexibility for administration in young children...
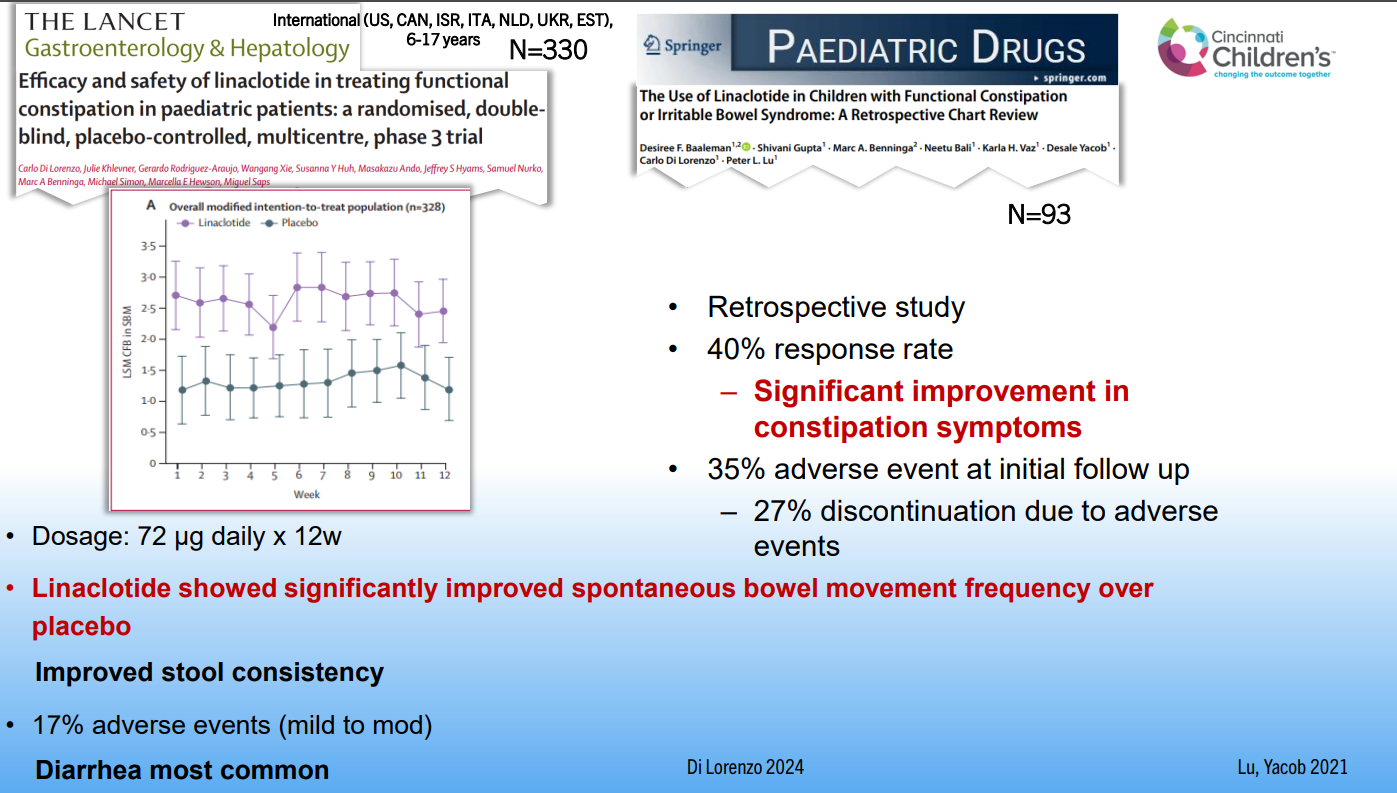
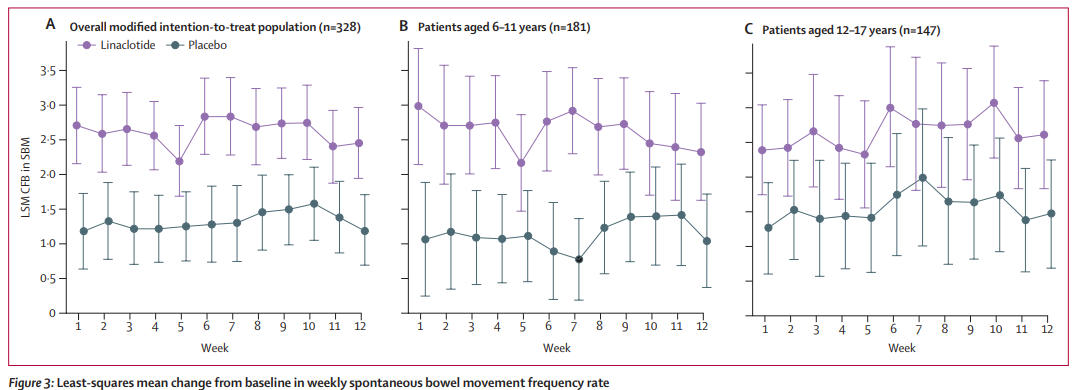
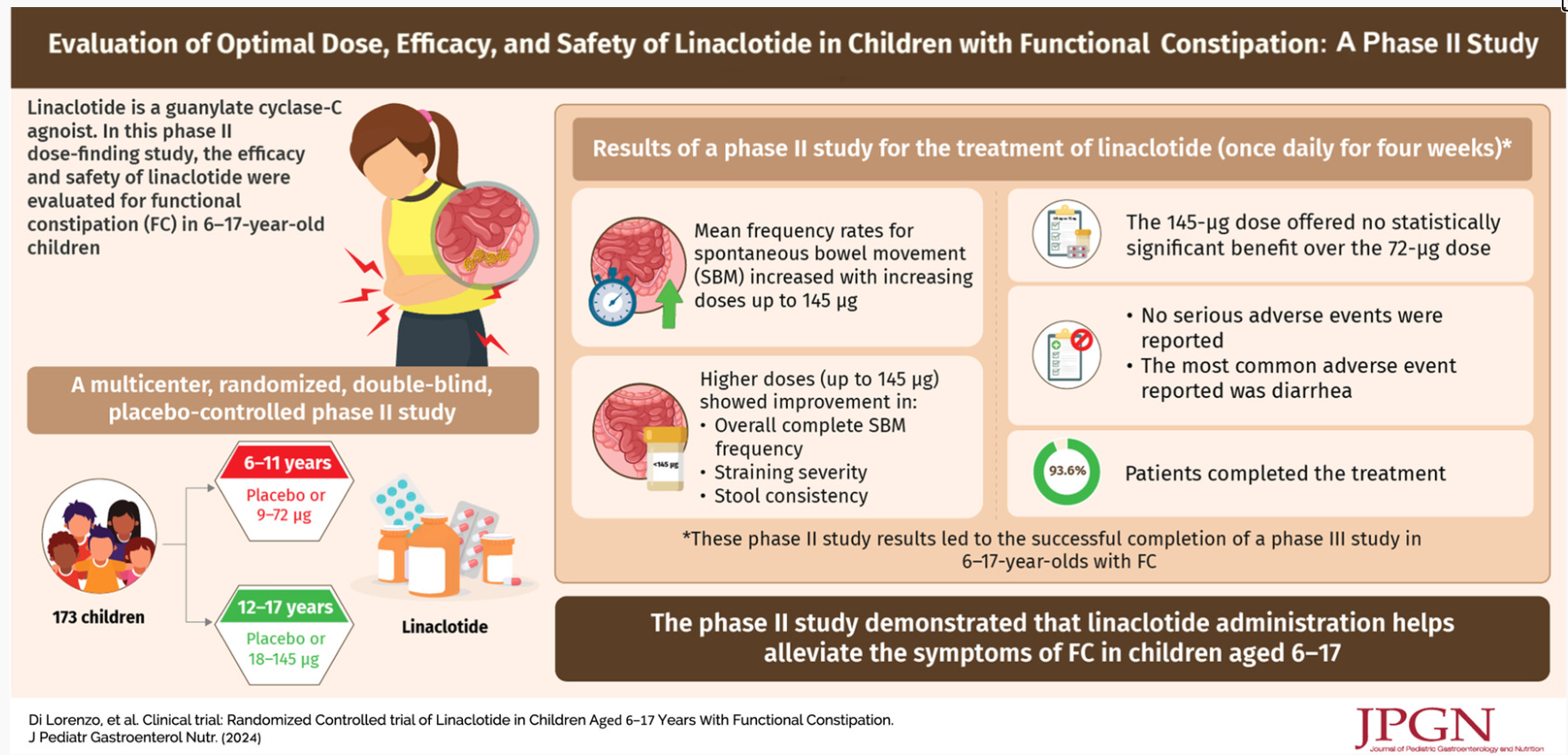
The FDA approval for pediatric patients ages 2-5 was supported by data from a 12-week Phase 3 randomized, placebo-controlled clinical trial evaluating LINZESS in pediatric patients aged 2-5 years with FC. In the study, LINZESS 72 mcg demonstrated improvement in spontaneous bowel movement frequency compared with placebo. The safety profile of LINZESS observed in the trial was generally consistent with the established safety profile from trials in adults with chronic idiopathic constipation (CIC) and older pediatric patients with FC...
LINZESS 72mcg is available as a once-daily treatment of FC for pediatric patients 2 years of age and older
My take: In this age group, typical over-the-counter laxatives including polyethylene gylcol, magnesium products, and senna products along with diet and behavior modification will be effective for most children. Most children will not need a prescription medication to manage their constipation.
Related blog posts:
- Linaclotide -Here’s the Pediatric Data (2024)
- Linaclotide -Now FDA-Approved for Children (2023)
- Willie Sutton and Refractory Constipation
- Meta-Analysis and Systemic Review: Efficacy of Drugs for Pediatric Constipation
- Position Paper: Pediatric Refractory Constipation Management
- What’s Wrong with Ordering an AXR for Constipation in the ER?