Before today’s post –more on voting this year:
Democracy Docket Four Ways to Safely Cast Your Ballot without USPS
- This article also has very helpful links to all of the states’ resources, regulations, and contacts
Several recent commentaries have shown scenarios impacted by this pandemic. Thanks to Ben Gold for sharing these references.
CA Wong et al. Pediatrics, July 2020, 146 (1) e20200973; DOI: https://doi.org/10.1542/peds.2020-0973. Full link: Mitigating the Impacts of the COVID-19 Pandemic Response on At-Risk Children
Here, we (1) highlight the health risks of the pandemic response measures to vulnerable pediatric subpopulations and (2) propose risk mitigation strategies that can be enacted by policy makers, health care providers and systems, and communities.
- Children With Behavioral Health Needs
- Children in Foster Care or at Risk for Maltreatment
- Children With Medical Complexity
R Cholera et al. Pediatrics. July 2020, 146 (1) e20201094; DOI: https://doi.org/10.1542/peds.2020-1094 Full link: Sheltering in Place in a Xenophobic Climate: COVID-19 and Children in Immigrant Families
One in 4 children (>18 million) in the United States lives in an immigrant family, in which the child or ≥1 parent was born outside the United States.1 Among children in immigrant families (CIF), >7 million live in “mixed-status” families, meaning ≥1 parent is not a US citizen.2… The COVID-19 pandemic amplifies existing inequities and introduces new ones as immigrant families navigate school closures, lack of health insurance and paid leave, and decisions to seek medical care or public services amid ongoing immigration enforcement. Additionally, immigrant families are more likely to live in multigenerational households,4 heightening the risk of COVID-19 for multiple family members…For CIF in US communities coping with persistent fears of immigration enforcement and family separation, economic devastation during a pandemic may threaten the stability of place. In this article, we apply a health equity framework5 to evaluate the impact of COVID-19 on CIF and highlight opportunities for advocacy and action for pediatricians, hospitals and health care systems, and policymakers to mitigate the unique risks faced by CIF
AM Evans et al. Pediatrics: July 2020, 146 (1) e20201163; DOI: https://doi.org/10.1542/peds.2020-1163. Full link: Pediatric Palliative Care in a Pandemic: Role Obligations, Moral Distress, and the Care You Can Give
Moral distress refers to the experience of being unable to take the action that one believes to be morally right or required.1… the inability to provide care because of resource constraints, involvement in care that one deems to be against a patient’s interests, and disputes about care planning with families and within teams…
We cannot have an obligation to save a life that cannot be saved: we can only be obliged to do what we can… It is only your role to act well within your scope of responsibility and to be the best clinician that you can be under the circumstances. Recognizing the limits of one’s powers can relieve a burden of guilt that is unconnected with one’s own choices and actions.
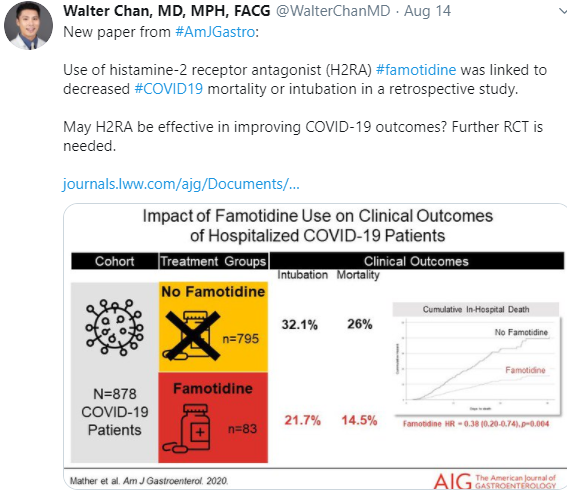
Famotidine may be helpful based on a retrospective study:
This long piece from Slate details the myriad public health mistakes in the U.S. approach to COVID-19: The Trump Pandemic