
L Chang. Gastroenterol 2021; 163: 1092-1098. How to Approach a Patient with Difficult-to-Treat IBS
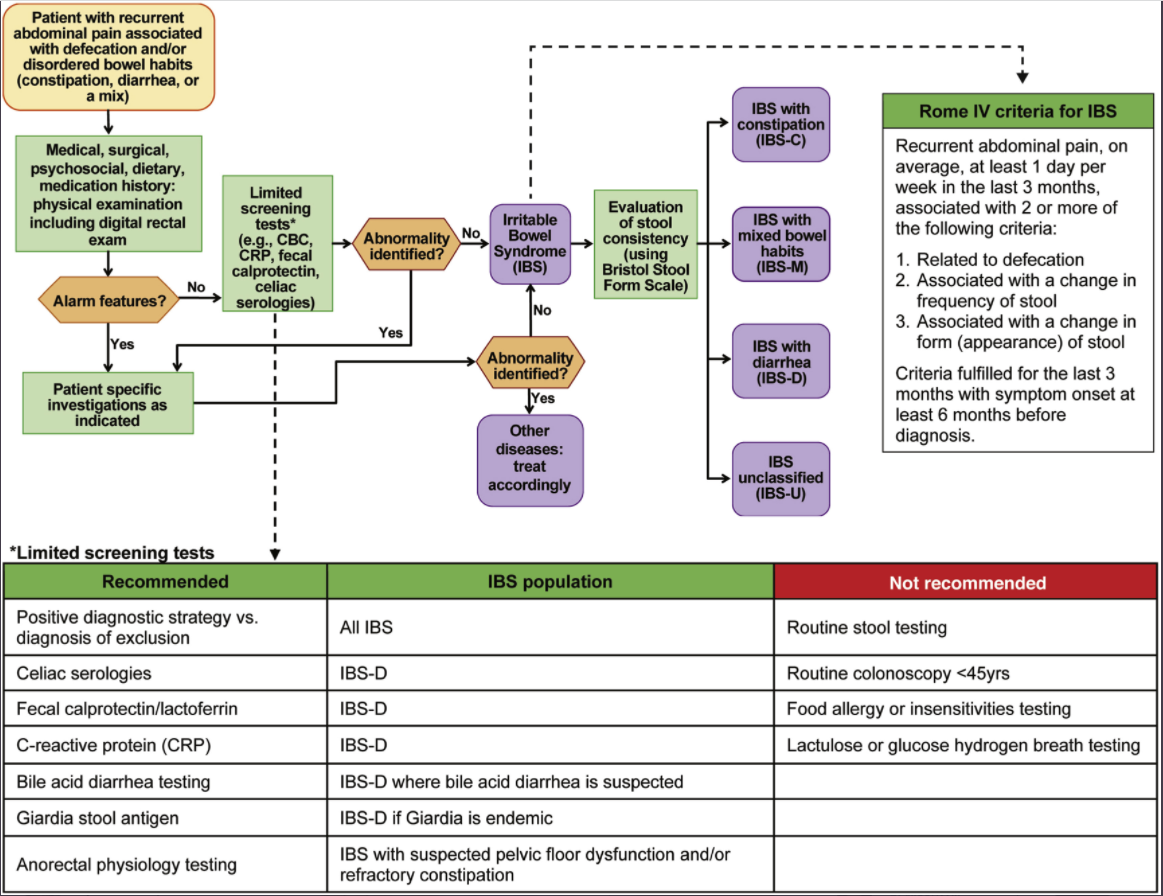
For a short article, this review provides a lot of practical advice. Challenges with IBS include the lack of objective biomarkers and “patients are often dissatisfied with a positive diagnostic approach or even after multiple negative tests.” The author recommends the following:
- Confidently communicate the diagnosis of IBS
- Explain visceral hypersensitivity and its associated with pain, and bloating and why central neuromodulators and behavioral therapy are often used. Explain that IBS can be associated with high-amplitude propagating contractures which can cause pain/diarrhea
- Treatment focused on ‘RESET’ =Relationship with patient-provider, Education/reassurance, Symptom assessment, Exacerbating/alleviating factors, and Targeting treatment (see Table 1)
Treatment may need to target gut, brain and/or both
- Dietary treatments considered 1st line approach
- Treatment pharmacology options for IBS-D include antidiarrheals, antispasmotics, rifaximin, eluxadoline, alosetron (rarely, can cause ischemic colitis), bile acid sequestrants
- Treatment pharmacology options for IBS-C include polyethylene glycol, lubiprostone, linaclotide, plecanatide, and tegaserod (restricted to women <65 yrs w/o cardiovascular dz)
- Treatment pharmacology options for all IBS include TCAs (start with low dose and can titrate upwards; amitriptyline for IBS-C, nortriptyline or desipramine for IBS-M or IBS-C), SNRI (eg. duloxetine (may be better than TCAs in patients with IBS-C and comorbidities like fibromyalgia and depression), mirtazapine (small studies demonstrated benefit for IBS-D and functional dyspepsia), SSRIs (“consider…in patients with predominant anxiety and/or depression…advise against its use as primary treatment for IBS w/o comorbid psychological disorder”), delta ligand agent (eg. pregabalin) (consider if refractory to other treatments), and brain-gut therapies (eg. CBT, GDH)
Related blog posts:
- Patient Information on Irritable Bowel (Rome Foundation)
- Mechanisms of IBS and Functional Pain (2021)
- Is There a Way to Prove Which Dietary Factors Trigger IBS?
- Advice on Abdominal Pain for Everyone Who Cares for Children | gutsandgrowth
- Brave New World: Psychotropic Medications and Pediatric Functional GI Disorders
- NY Times: “Millions Take Gabapentin for Pain. But There’s Scant Evidence It Works.” | gutsandgrowth
- A 6-Year Study of Amitriptyline, Escitalopram, and Functional Dyspepsia
- Advice on Abdominal Pain for Everyone Who Cares for Children | gutsandgrowth
- Does buspirone help functional dyspepsia?
- How Effective are the Treatments for Functional Abdominal Pain? | gutsandgrowth
- Will I Have This Stomach Pain Forever? (Part 1) | gutsandgrowth
- FODMAP diet -Real World Experience
- Pregabalin Helpful for Functional Dyspepsia (Small Study)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
