Recently, Dr. Valeria Cohran gave our group a terrific update on Short Bowel Syndrome (SBS)/Intestinal Failure (IF). My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of her slides. Dr. Cohran has been a leader in intestinal rehabilitation. Among many accomplishments, she was the 2025 recipient of the 2025 Margaret Stallings NASPGHAN Distinguished Service Award.

Key points:
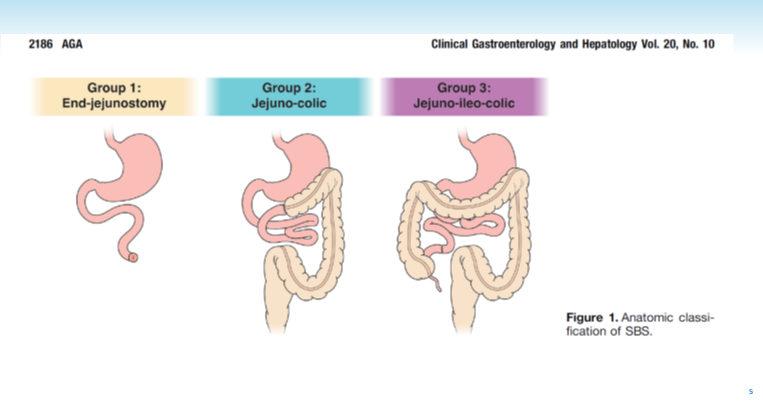
- Most children with SBS/IF are able to taper off parenteral nutrition (PN). Even ~30% of those with extreme SBS (<10% of expected bowel length) are able to achieve enteral autonomy.
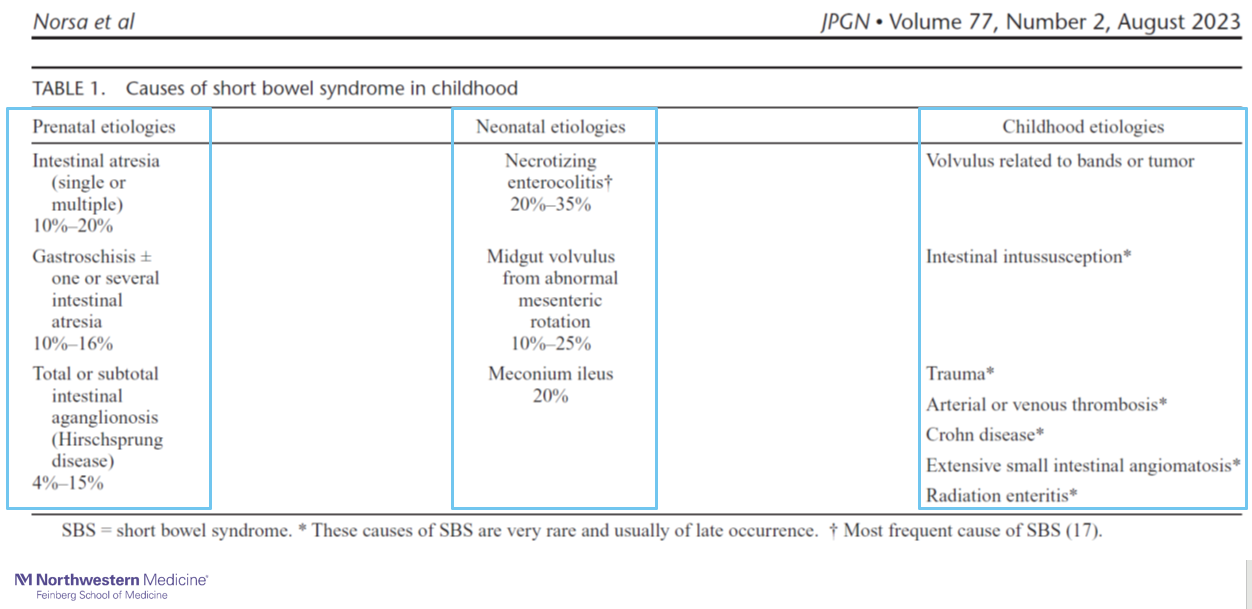
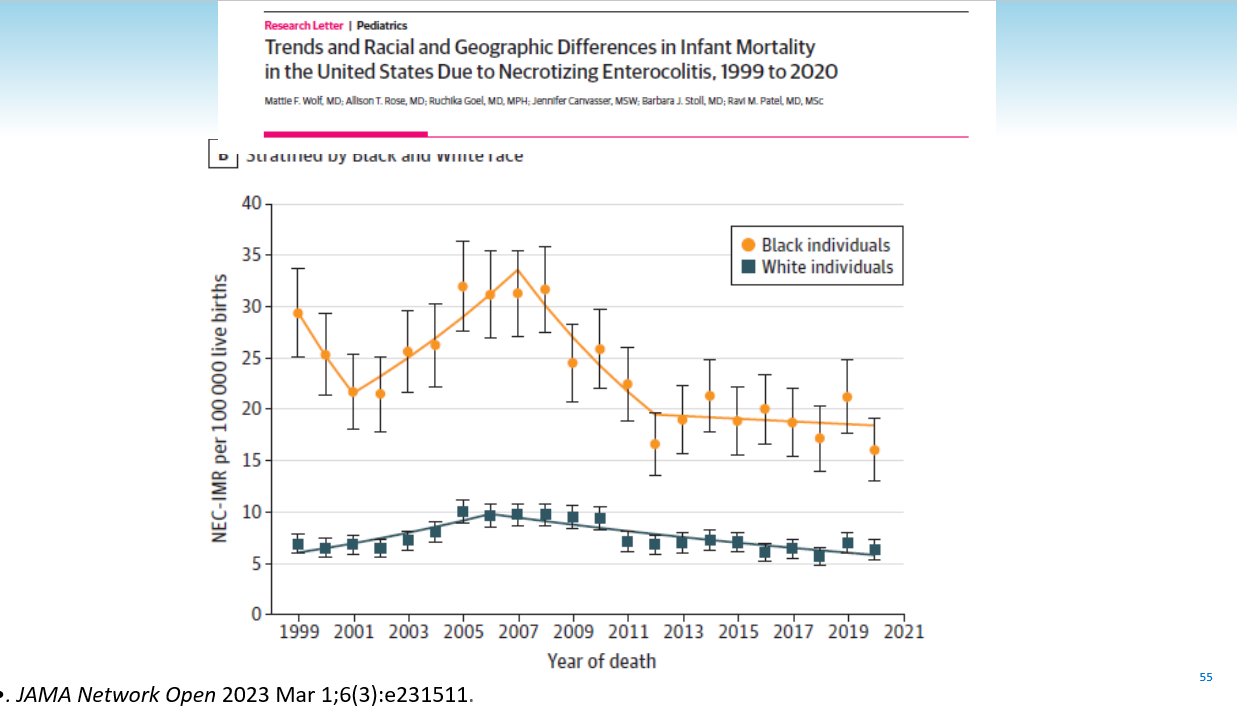
- SBS/IF due to NEC has a generally more favorable outcome than other etiologies
- Stoma takedown is associated with better outcomes (eg. more likely to taper off PN). (Raghu et al. JPEN. 2023;47:1047-55). Taking down stoma may be beneficial if unable to taper PN and in those developing liver disease
- SBS/IF caretakers spend a median of 29 hrs/week managing PN, enteral nutrition, medications, and other tasks
- In the nursery, one study reported that NICU patients with IF spent a median of 150 days and cost more than $500K
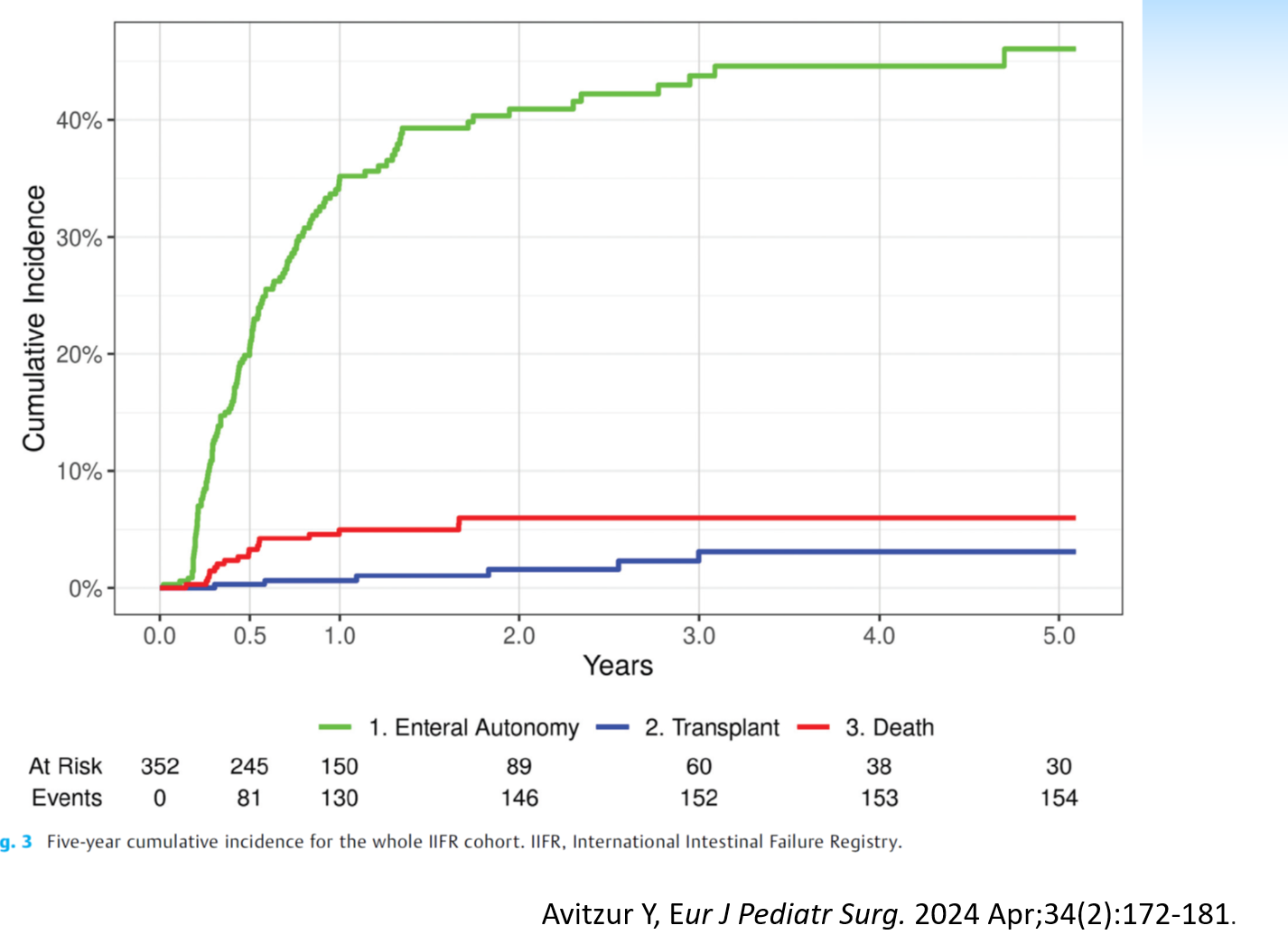
- Overall, advances in SBS/IF management have been associated with lower death rates and lower intestinal transplant rates (~30 ITx last year), yet similar rates of achieving enteral autonomy





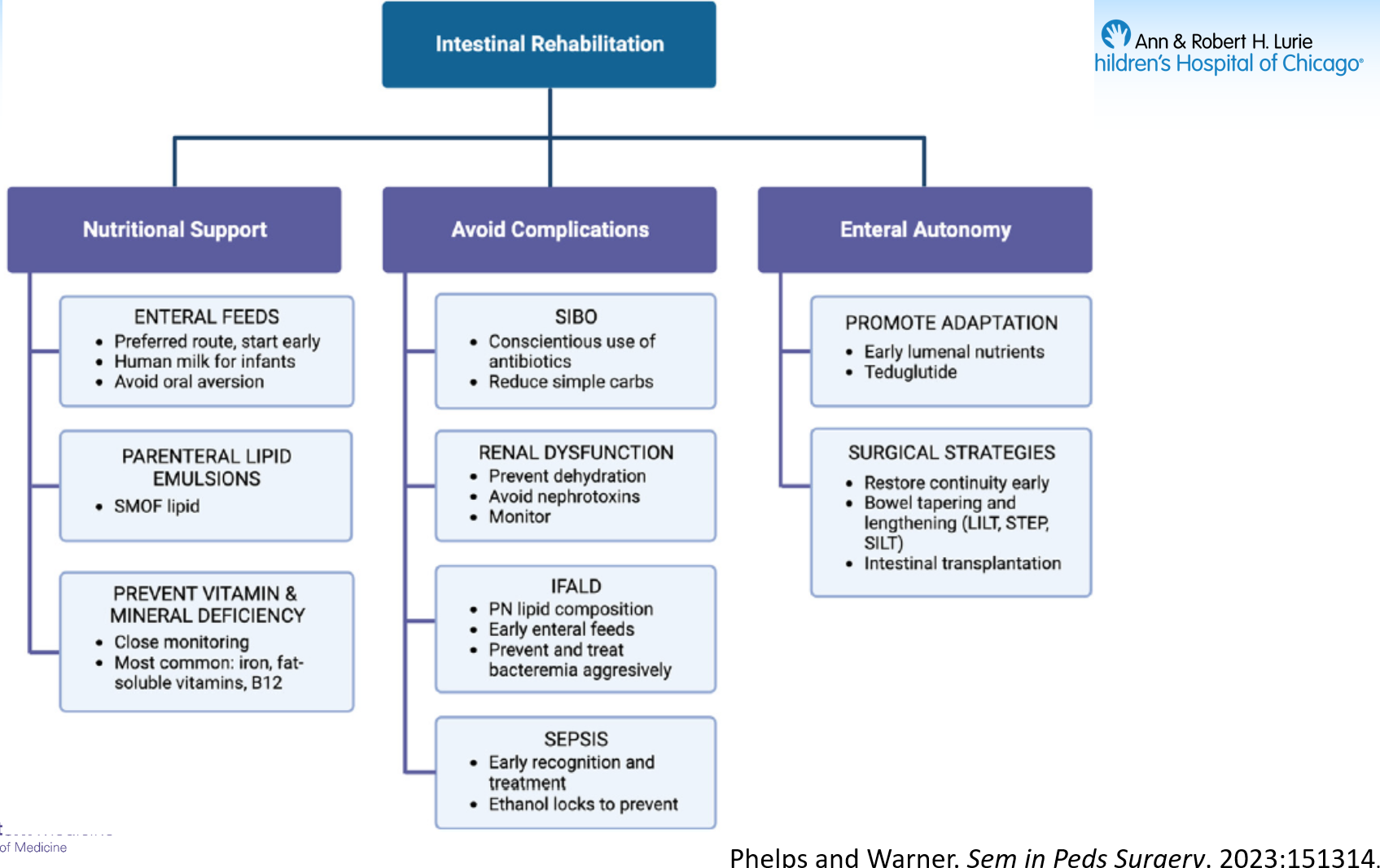
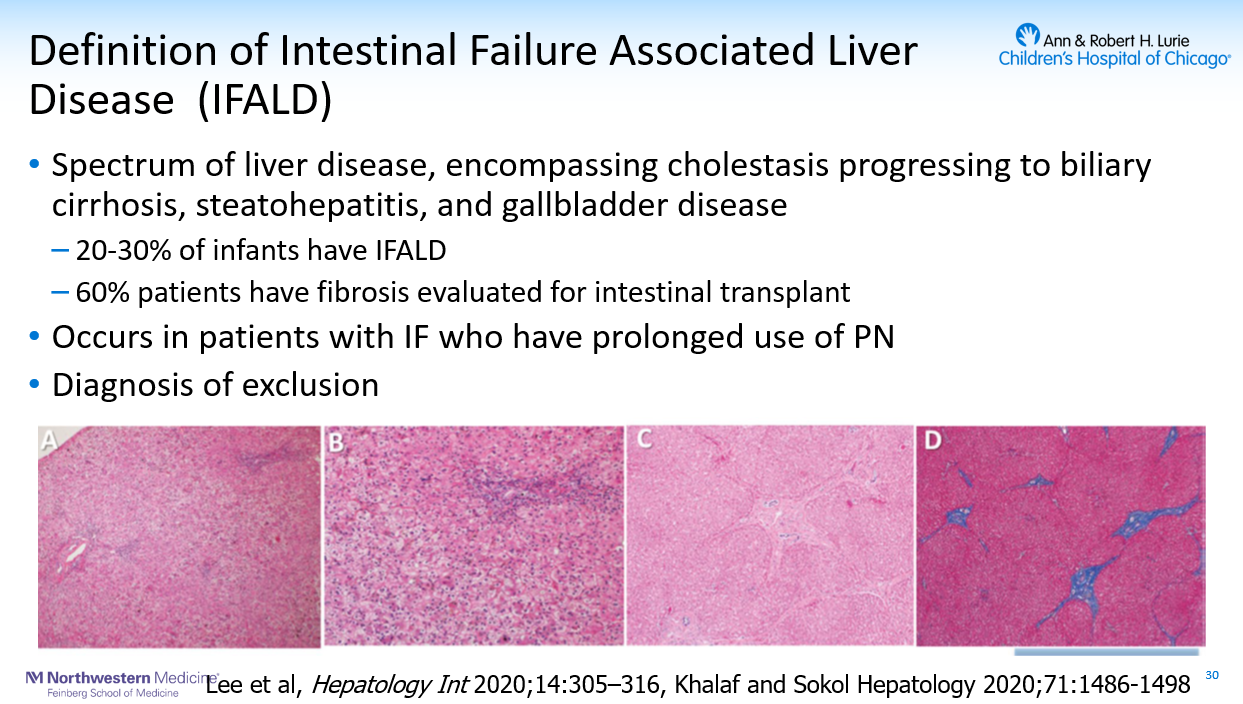

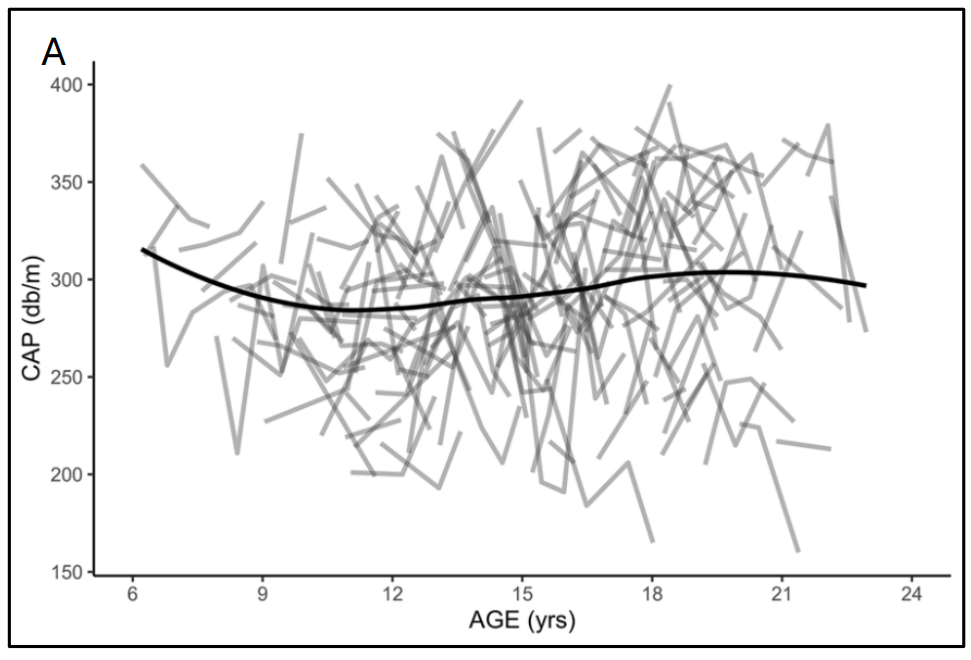
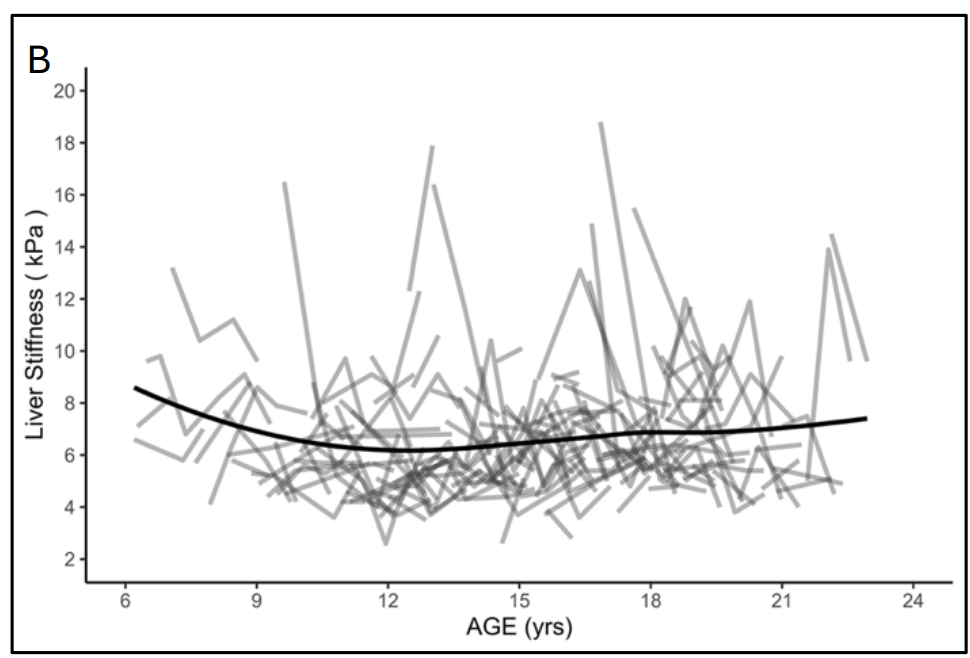
- Fish oil based lipid emulsions do not always work; cirrhosis can still develop even with minimal biochemical marker alterations
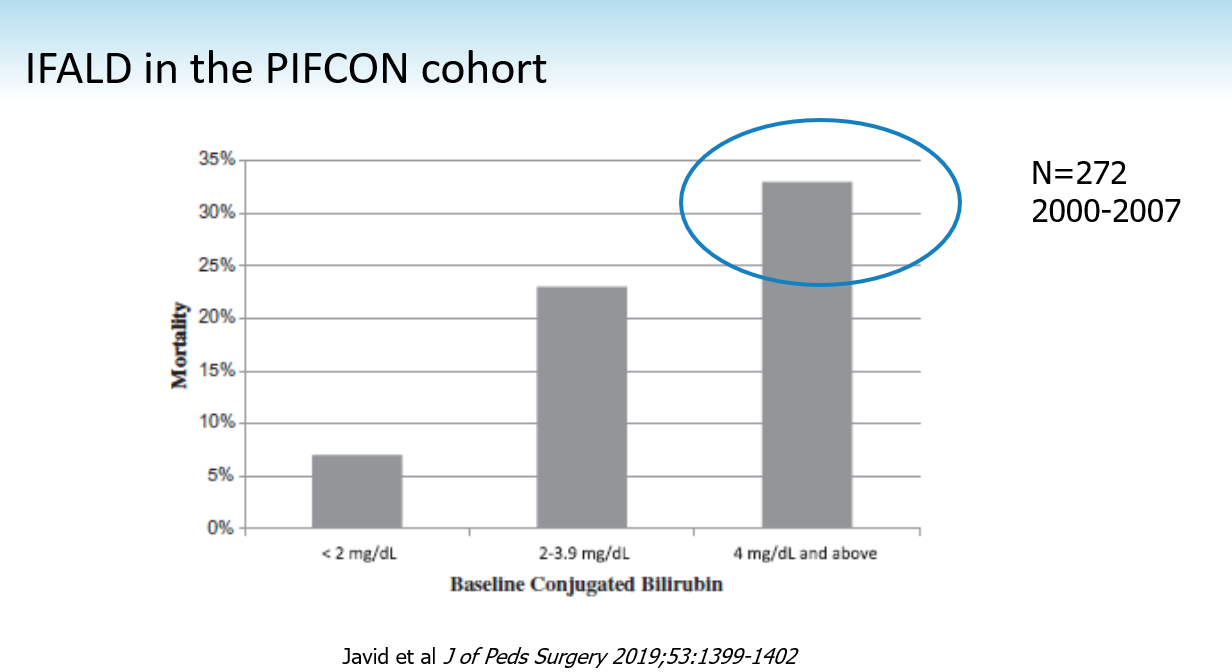
- IFALD mortality is associated with degree of conjugated hyperbilirubinemia, though we are not seeing this complication much with current management

- GLP-2 can reduce PN requirements by more than 20% in the majority of those with SBS/IF and may help achieve enteral autonomy in about 20%. However, their use requires close monitoring for fluid overload and electrolyte disturbances

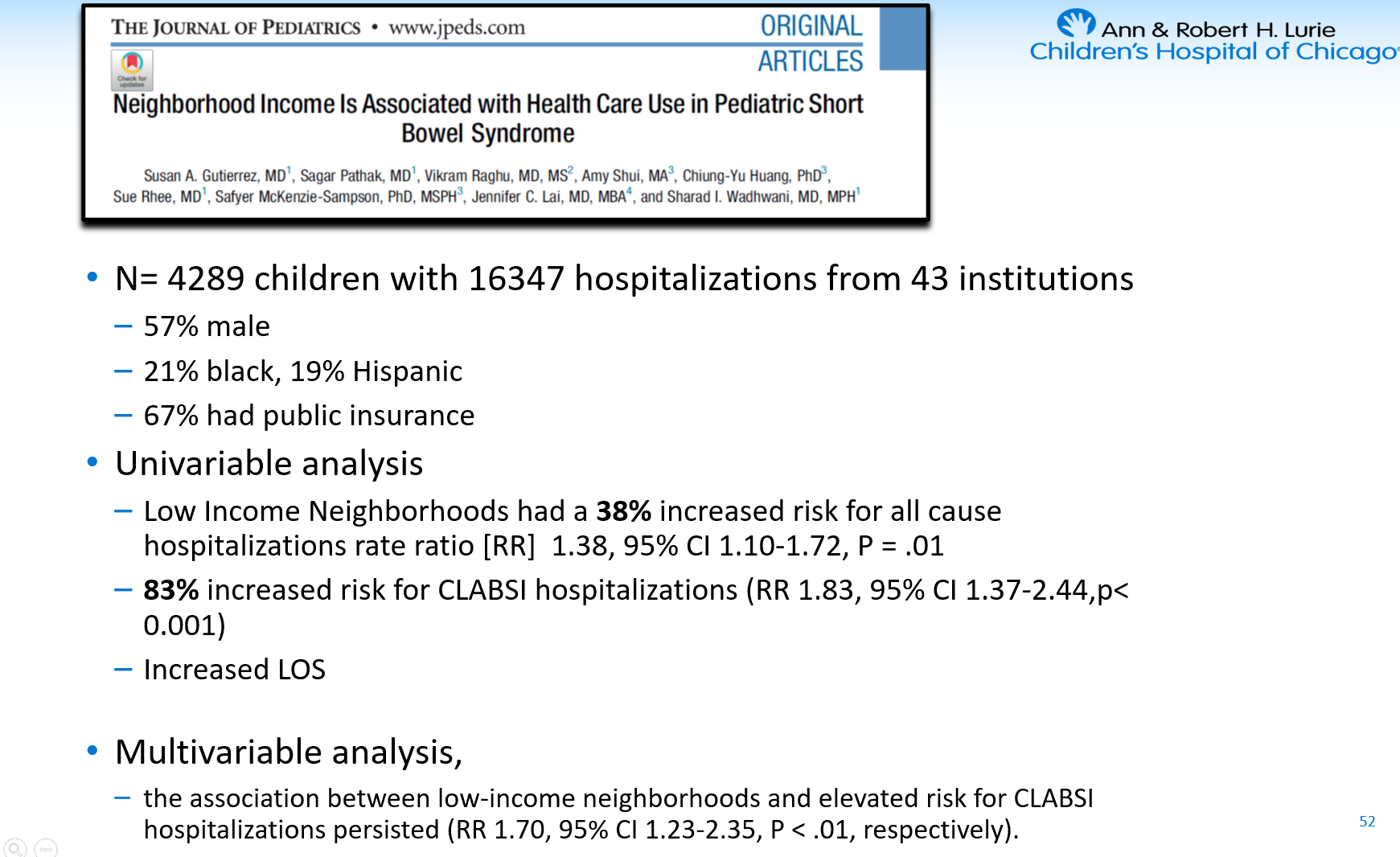
- Lots of disparities noted along socioeconomic variables. For outpatient management, home nursing care is not available in some neighborhoods


Related blog posts:
- Dr. Danielle Wendel: Management of Short Bowel Syndrome
- Practical Intestinal Rehabilitation (Part 1)
- Practical Intestinal Rehabilitation (Part 2)
- Short Bowel Syndrome is a Full Time Job
- Income and Health Outcomes in Pediatric Short Bowel Syndrome
- Long-Acting GLP-2 Analogue Glepaglutide Reduces Parenteral Support
- Is GLP2 Worth $300K per Year?
- Polyurethane vs Silcione with Ethanol Locks
- Management of Ostomies
- Aspen Webinar 2021 Part 4 – IFALD Update
- Personal Account of Extreme Short Bowel Syndrome