
Hoskins BJ, Ng K, RexDK. J Pediatr GastroenterolNutr. 2025;81:162‐166. Open Access! Is it time to revisit the need for pediatric polypectomy guidelines?
This commentary/review makes a number of useful points:
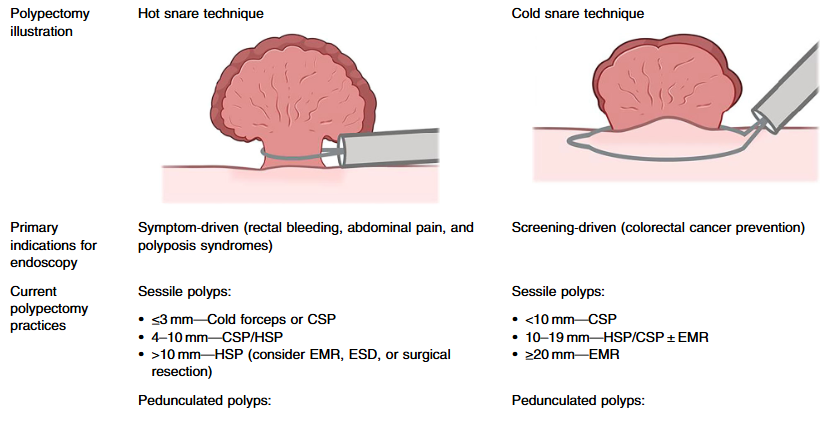
- In adults, there have been important changes in recommendations. Guidelines recommend “cold snare polypectomy (CSP) for small and diminutive polyps (<10 mm) due to its favorable safety profile compared to electrocautery techniques.2”
- “The European Society for Paediatric Gastroenterology, Hepatology, and Nutrition provides position papers for polyposis syndromes from 2019, including familial adenomatous polyposis (FAP), Peutz–Jeghers syndrome (PJS), and juvenile polyposis syndrome (JPS), which also provide guidance on polypectomy practices.8–10“
- “No studies have directly compared the safety and efficacy of various polypectomy techniques—such as cold forceps, hot forceps, cold snare, and hot snare methods—in children. As a result, pediatric practices often rely on extrapolated adult data, despite key differences in patient populations.”

My take (borrowed from authors): “Polypectomy is central to pediatric endoscopy, yet evidence-based, pediatric-specific guidelines are lacking.”
Related article: Hoskins BJ, Grabau JM, Rex DK. J Pediatr Gastroenterol Nutr. 2025;81:1311-131. Pediatric endoscopic mucosal resection: a 10-year single-center experience. . https://doi.org/10.1002/jpn3.70194
Related blog posts:
- Cold vs Hot Polypectomy for Small Polyps (2023)
- How to Do a Colonoscopic Polypectomy & U.S. COVID-19 Tracker
- How Benign Are Juvenile Polyps?
- Adverse Events Following Pediatric Endoscopy -Previously Underestimated
- ESPGHAN Juvenile Polyposis Position Paper While the polyps described are not tubular adenomatous polyps, it is noted that guidelines in adults recommend followup in 5-10 years for a single (non-serrated) adenomatous polyp (Polyps: Clinical Decision Tool).
- Updated Guidelines on Genetic Testing/management for Hereditary GI Cancer Syndromes
- Surprising Genetic Mutations in Polyposis Study
- Polyposis in Pediatric Patients -Review
- Consensus guidelines after polypectomy | gutsandgrowth)
- Adenoma Detection Rate: Life or Death Quality Measure
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition

