
A Porto et al. JPGN Reports. 2026;7:59–63. Open Access! Feasibility and clinical value of pyloric functional luminal imaging probe in an infant
Case report: “This case highlights the feasibility, safety, and clinical effectiveness of FLIP as a diagnostic and treatment tool in an infant with pyloric dysfunction.”
In brief, the authors describe a former 26 week premature infant with gastric dysfunction with gastric output >100 mL/kg/day while on GJ feeds. “His history was notable for necrotizing enterocolitis with multiple intestinal perforations and bowel resections with resultant short bowel syndrome (97 cm small bowel, intact colon) and chronic respiratory failure requiring tracheostomy and mechanical ventilation.” After obtaining FLIP measurements, IPBI (intrapyloric botulinum toxin injection) was performed with 100 international units of botulinum toxin A. Esoflip dilatation was performed using a 20 mm balloon. This led to full tolerance of gastric bolus feeds. When symptoms recurred, repeat IPBI and dilatation were performed with resolution of symptoms.
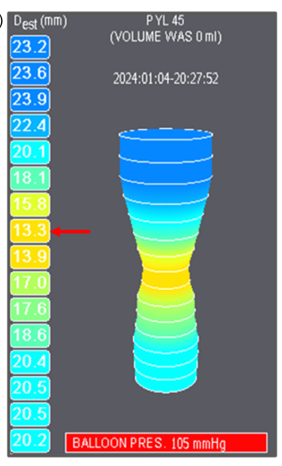
Max diameter 13.3 mm (arrow) at 45 mL balloon inflation
My take: I am not an expert on FLIP; however, it does not appear to be needed in this situation. Many practitioners would recommend botox injection with or without dilatation in patients with this type of presentation without using FLIP. The authors acknowledge that there are a “lack of reference values for infants” which makes FLIP interpretation more subjective.
Related blog posts:
- Botox for Pediatric Gastrointestinal Disorders
- Is Manometry Useful to Determine if Botox Will Help Nausea/Vomiting?
- Provocative Study: Pyloric Botox for Feeding Difficulties
- How Reliable is a Motilist in Interpreting Manometry and FLIP Studies?
- FLIP Patterns for Adults with Eosinophilic Esophagitis
- Using FLIP
