K Switkowski et al. The Journal of Pediatrics, 2026; 294. Open Access! Associations of Colic and Excessive Crying in Infancy with Food Allergy Outcomes in Childhood and Adolescence
Background: The authors have previously observed “increased risks of eczema, allergic rhinitis, and asthma throughout childhood and adolescence among children with a history of infant colic compared with unaffected infants.14“
Methods: Prospective study of 1263 generally-healthy participants with parent-reported food allergy from early childhood through mid-adolescence using multivariable logistic regression. In a subset (n = 242) with available biomarkers, the associations of colic with food-specific IgE sensitization in early childhood were examined.
Key findings:
- “In early childhood, 10% of children in Project Viva had a food allergy reported by their mothers. Peanut or tree nut allergies were most prevalent (6%), followed by cow’s milk (4%) and egg (2.5%) allergies”
- “Participants who had colic (25%, n=320) had a greater risk of any food allergy in early childhood than those unaffected by crying or colic (13% vs 8%; OR 1.7)”
- “The risk of current milk and egg allergies in early childhood also was greater for those who had colic as infants vs those unaffected (OR for milk allergy: 1.8)”
- “In early adolescence, the colic group had 2.1 times the risk of peanut allergy (8% vs 4%) vs the unaffected group”
- “In the subset with IgE, the colic group had 2.5 times the risk of early childhood IgE sensitization to peanuts compared with the unaffected (22% vs 11%).” However, none of the other foods had significant IgE sensitization: Cow’s milk OR 0.7, Egg white OR 0.5, Wheat OR 1.1, Soy OR 1.9, Sesame OR 1.4, Any IgE sensitization OR 0.8
Discussion Points:
- The authors “do not believe that colic itself is a cause of later food allergy but rather could be an early marker of greater risk for developing food allergy…these findings argue against characterizing colic as a benign, transient, and self-resolving condition as some have suggested.”
- Preventive measures should be implemented. “Early and consistent exposure to potential allergens at specific critical windows of life, particularly among high-risk children, is now known to be effective in promoting allergen tolerance and preventing the development of food allergy.3“
- Study limitations:
- “Parent-reported food allergies [were used] to define this outcome and acknowledge that this may involve some misclassification of outcome status if parents report allergies that have not been clinically validated.” Though, in a previous study, the “overall agreement between parent-reported and clinician-documented allergy status” was 98%.
- There was no data indicating whether food introduction in infants with colic was different than other infants.
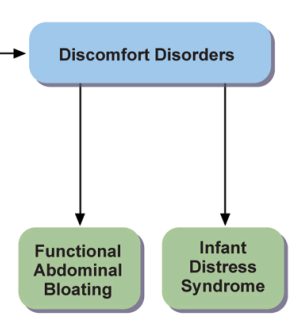
My take: It is unclear to me whether colic (now labeled Infant Distress Syndrome) is a true risk factor for later atopic diseases. It is possible that the presence of colic could increase the use of more elemental formulas and postpone food introduction which could increase the risk of food allergies.
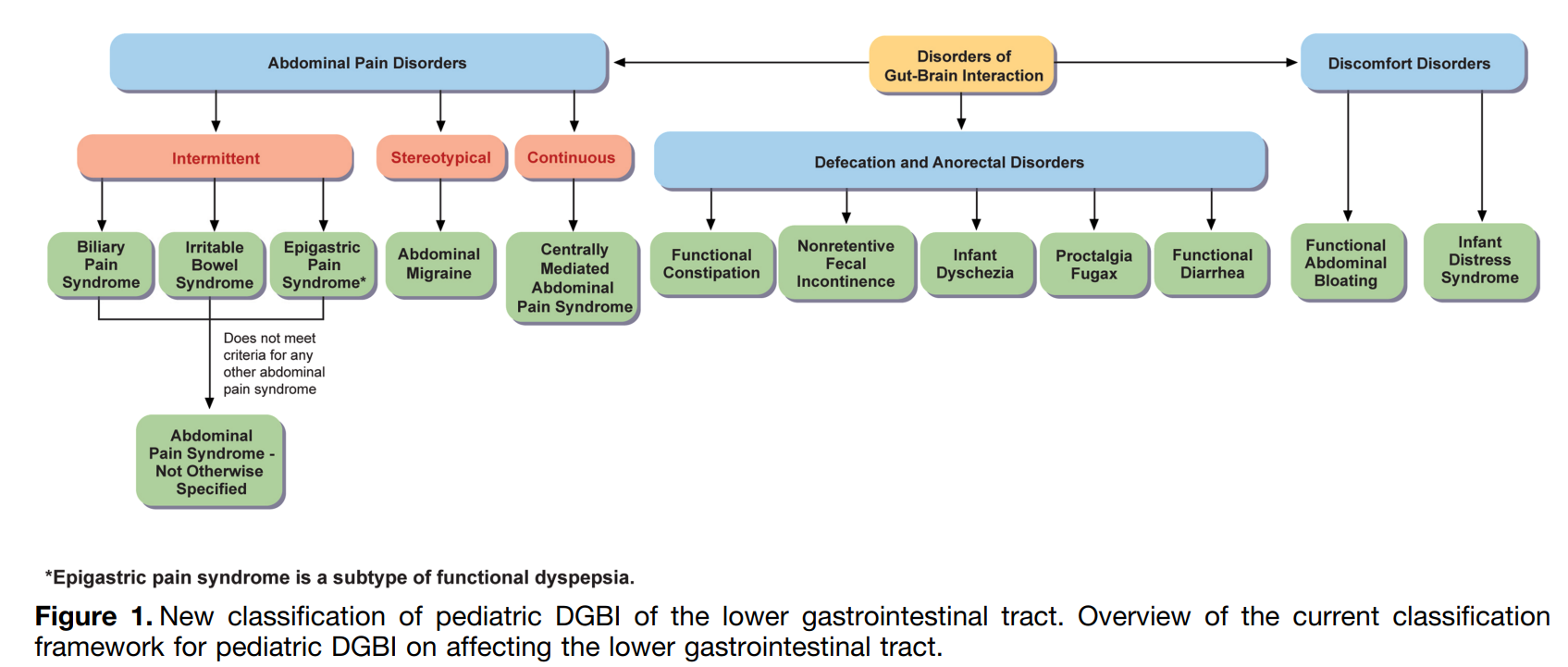
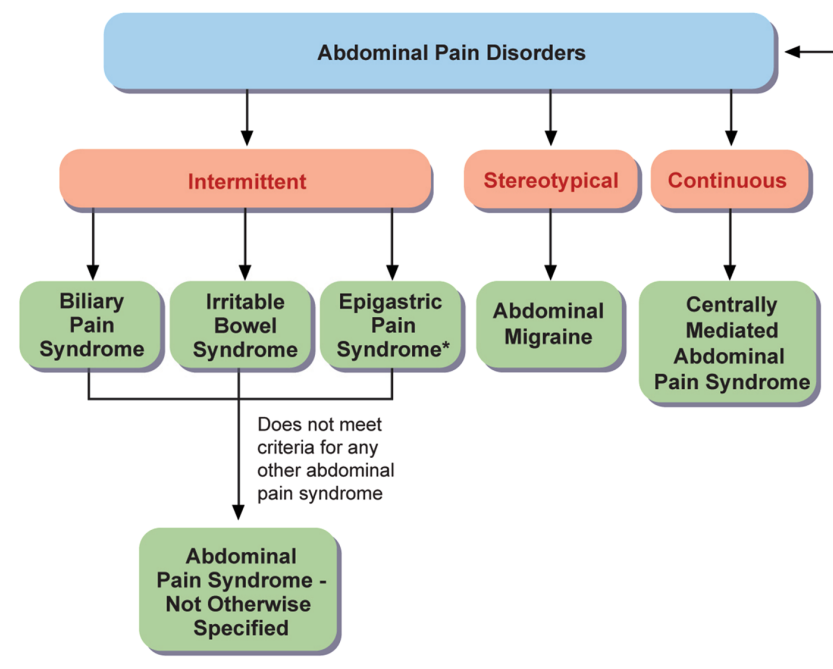
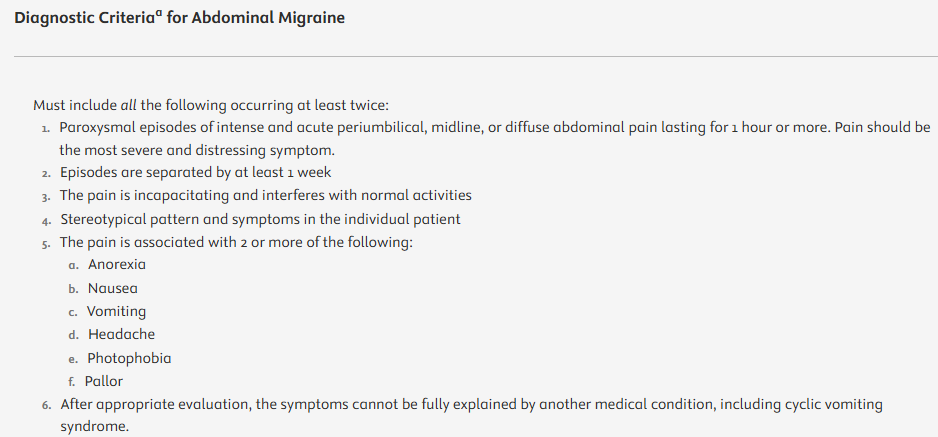
Related blog post: Rome V: Lower GI Tract and Biliary Disorders of Gut-Brain Interaction in Pediatrics (Part 1)