
Dr. Jose Garza joined our group in 2013 and has been providing excellent care for children throughout the South with suspected motility disorders. Recently, he gave our group a fabulous update on what’s new in motility. My notes below may contain errors in transcription and in omission. Along with my notes, I have included some of his slides. His talk had 123 slides; true motilists would be appalled that I haven’t included more of the high resolution tracing slides (though there are a few tomorrow).
Reflux:
- Positioning babies does not improve reflux (related post: Does Positioning Help Infants with Reflux?)
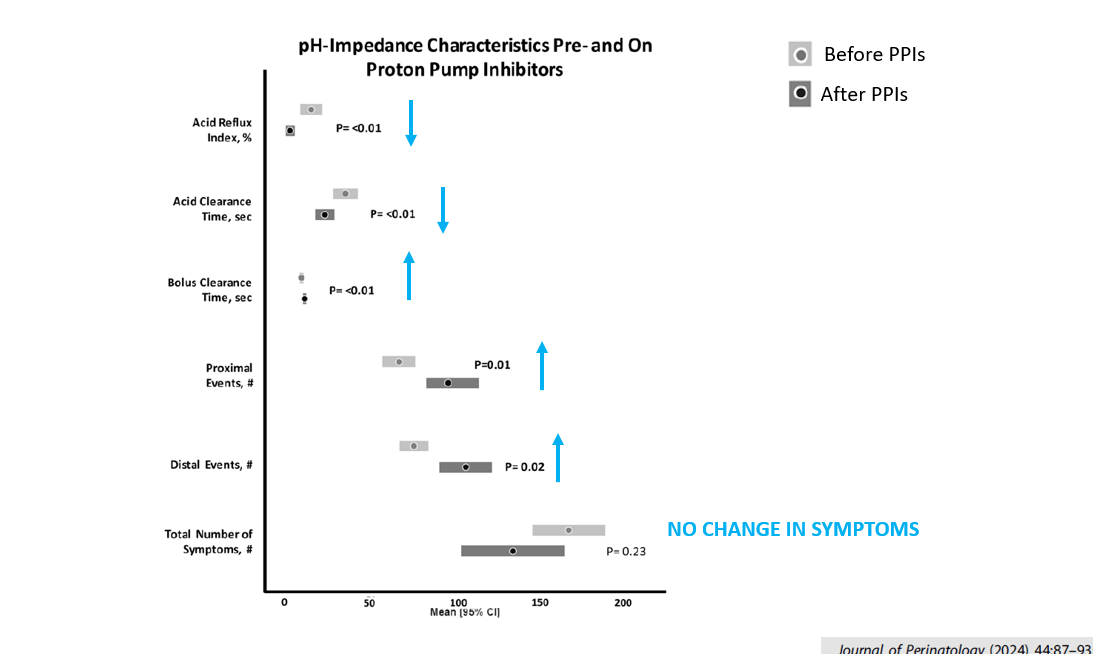
- NICU study of PPIs showed that in patients in which PPIs were continued had more trouble clearing reflux boluses than in children taken off PPIs
- PPIs may worsen oropharyngeal sensory mechanisms in infants
- Related post: Arching in Infants Not Due to Reflux

Colic:
- Colic may be a biorhythm disorder. Infants with colic sleep less and have family history with much higher rates of maternal migraines (related post: Is Infantile Colic a Biorhythm Disorder?)
BRUE:
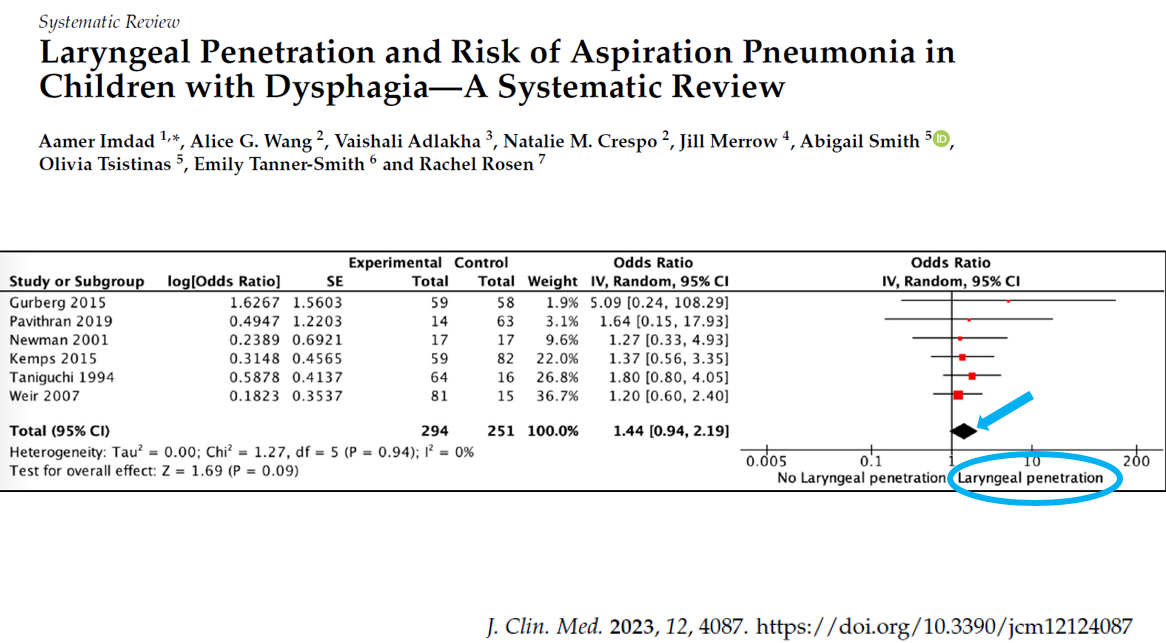
- 1 of 4 infants with GERD symptoms have oromotor discoordination (related post: Incredible Review of GERD, BRUE, Aspiration, and Gastroparesis)
- BRUE likely related to oromotor discoordination rather than GERD (related post: Blaming Reflux for BRUEs -Not Changing Despite Guideline Recommendations)

Laryngomalacia/Thickening:
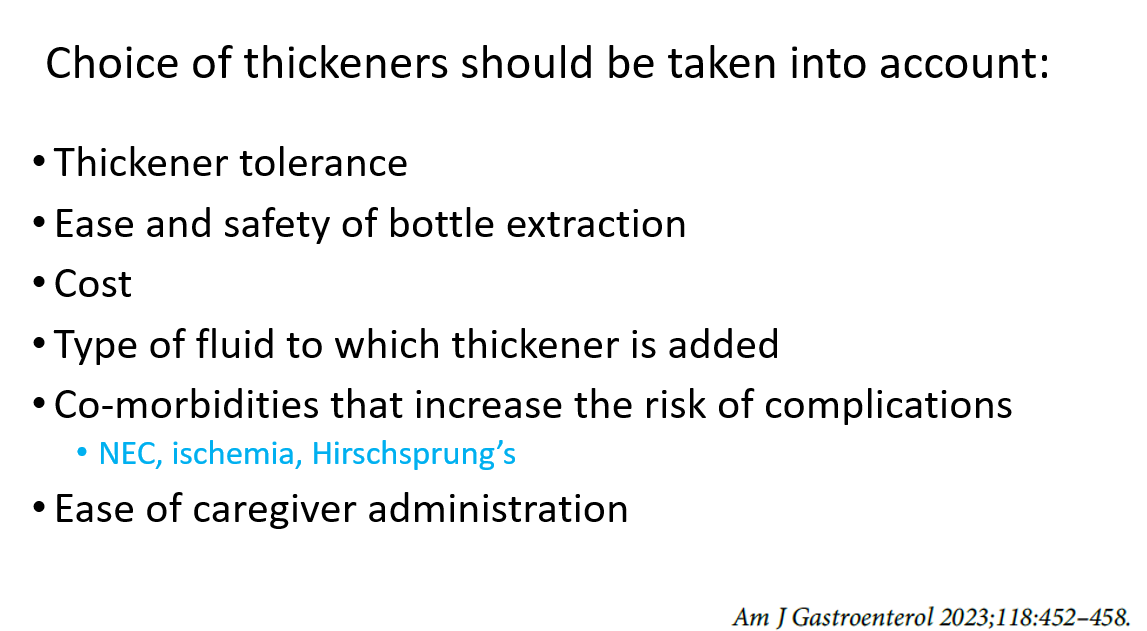
- Thickening helps reduce symptoms and hospitalizations
- Thickening can be tricky. Hard to thicken breastmilk and elemental formulas
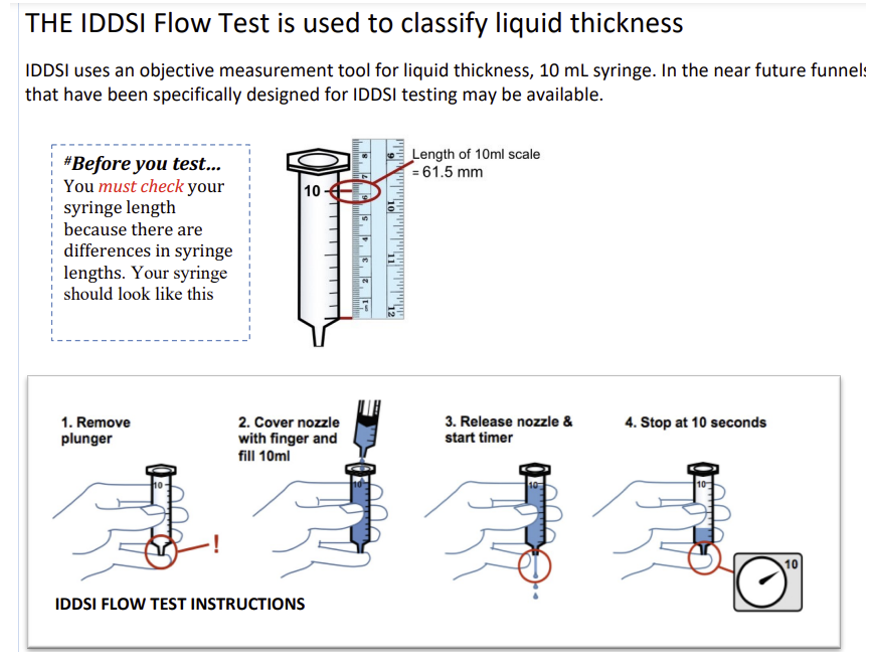
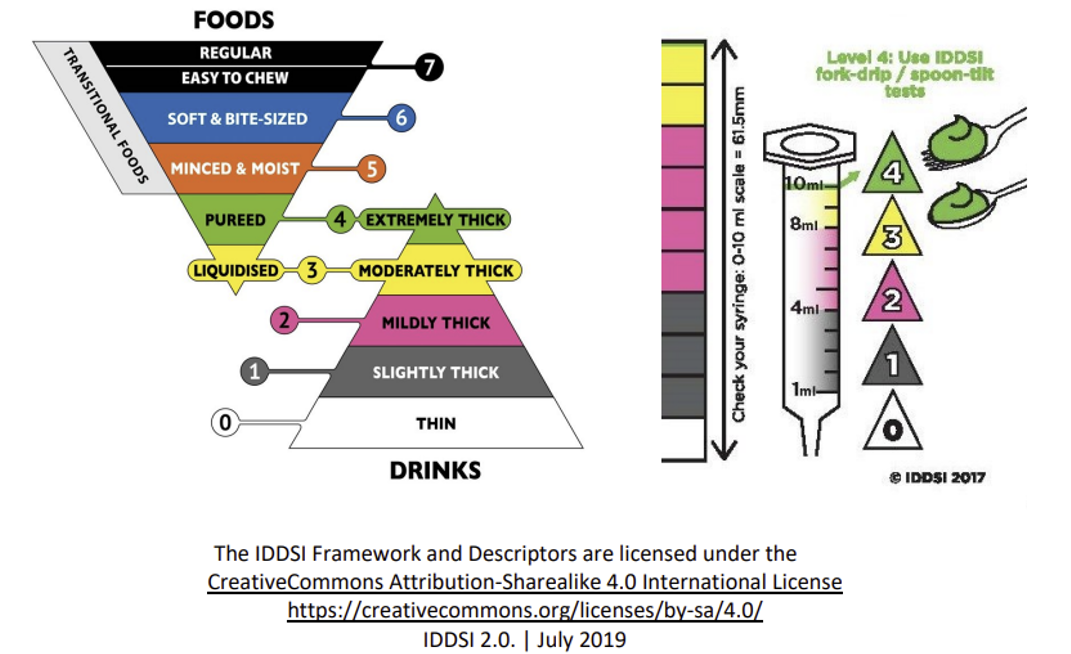
- IDDSI 10 mL Syringe Flow testing can determine if thickening is at desired level
- Related post: Acid Suppression for Laryngomalacia -Handed This Article to My ENT Colleagues
Impedance
- Predicts mucosal disease in the esophagus (and airway) (related post: Understanding Reflux/Airway Disease and Potential Role of Airway Impedance)
- In adults, but not pediatrics, balloon-based impedance technology has been useful in distinguishing GERD, EoE from normal mucosa
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.









