S Khanna et al. Gastroenterology, 2026 (In press). Open Access! AGA Clinical Practice Update on Management of Clostridioides difficile Infection in Inflammatory Bowel Disease: Expert Review
Best Practice Advice Statements
- In patients with IBD who have new or worsening diarrhea, CDI should be excluded, especially among those with colonic involvement, as they are at increased risk of CDI. Clinicians should consider and treat CDI in patients with end ileostomy or ileo-anal pouch anastomosis with worsening diarrhea.
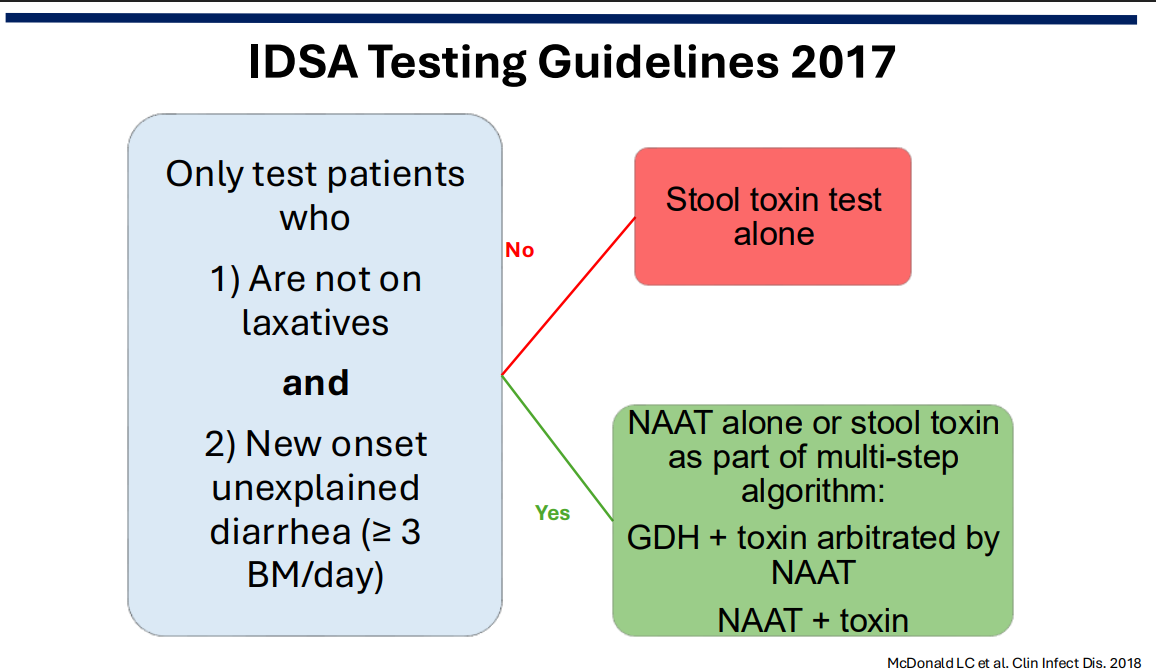
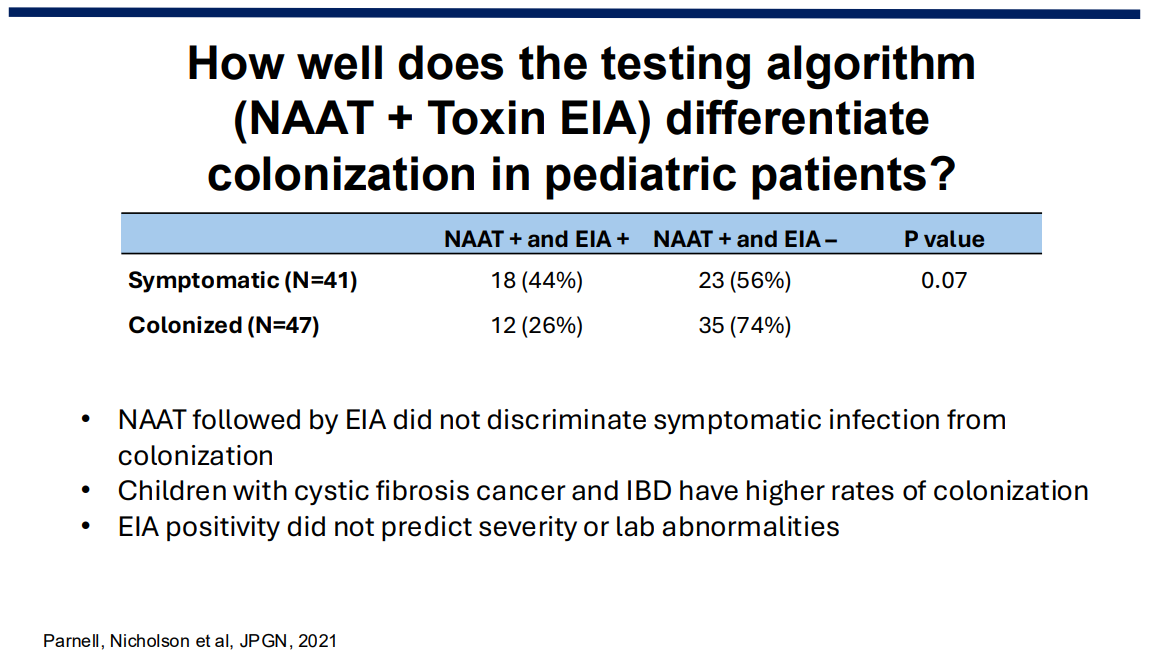
- In patients with IBD and suspected CDI, a multistep toxin-based assay should be used for diagnostic evaluation.
- In patients with IBD and recent CDI who have been treated successfully with antibiotics, recurrent diarrhea should prompt retesting for CDI.
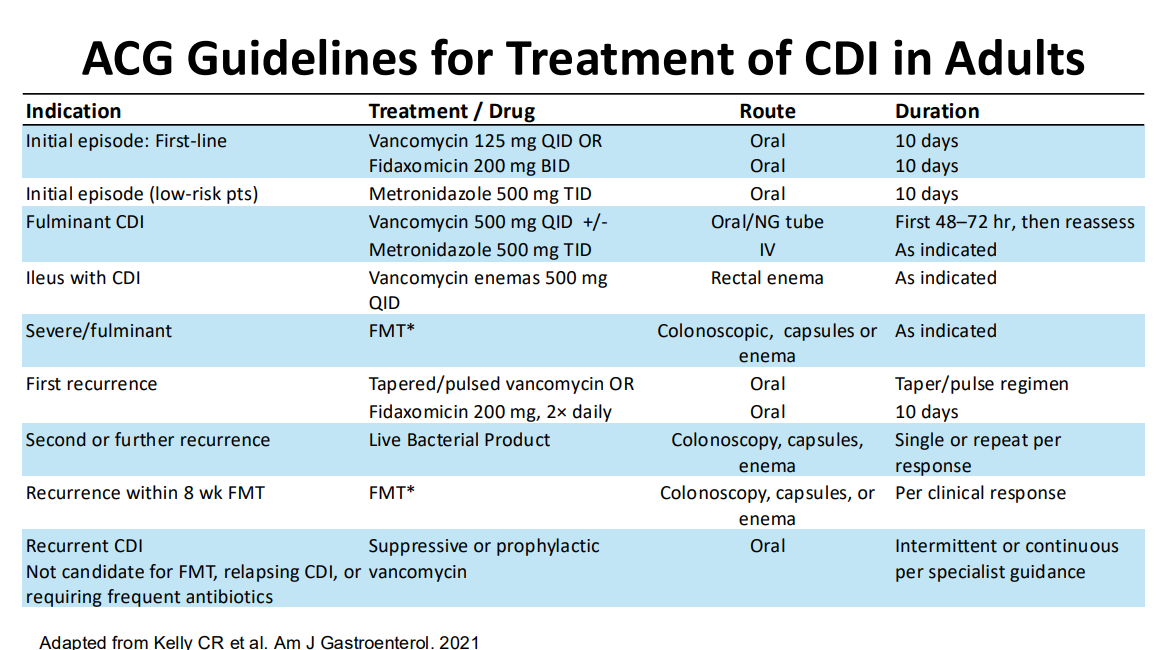
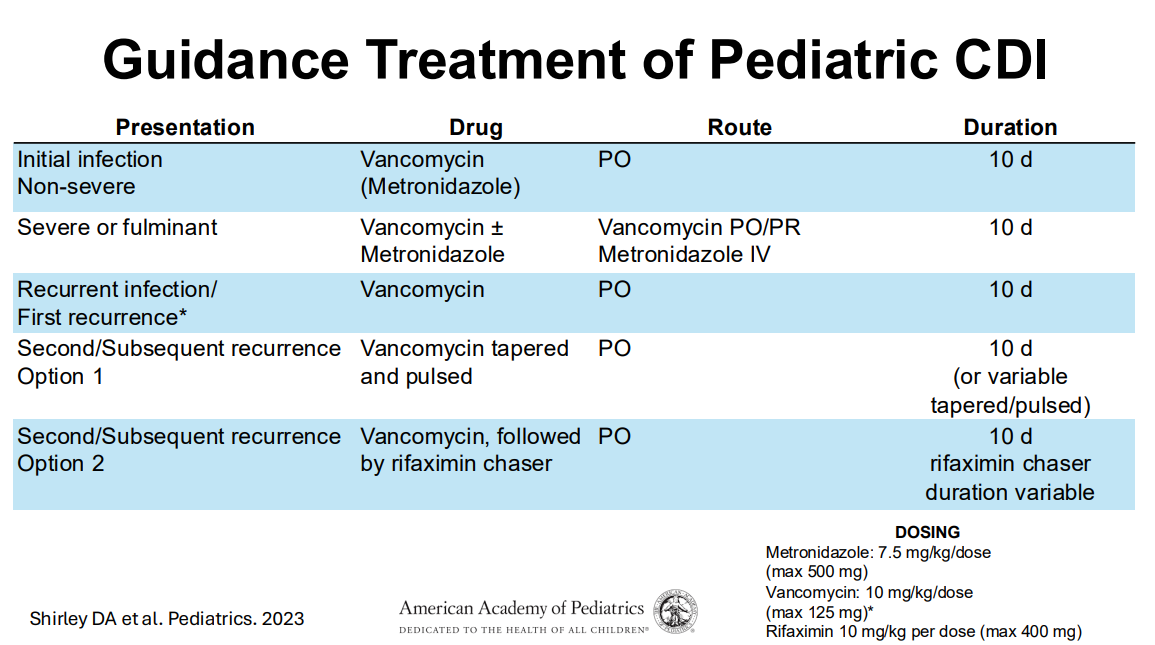
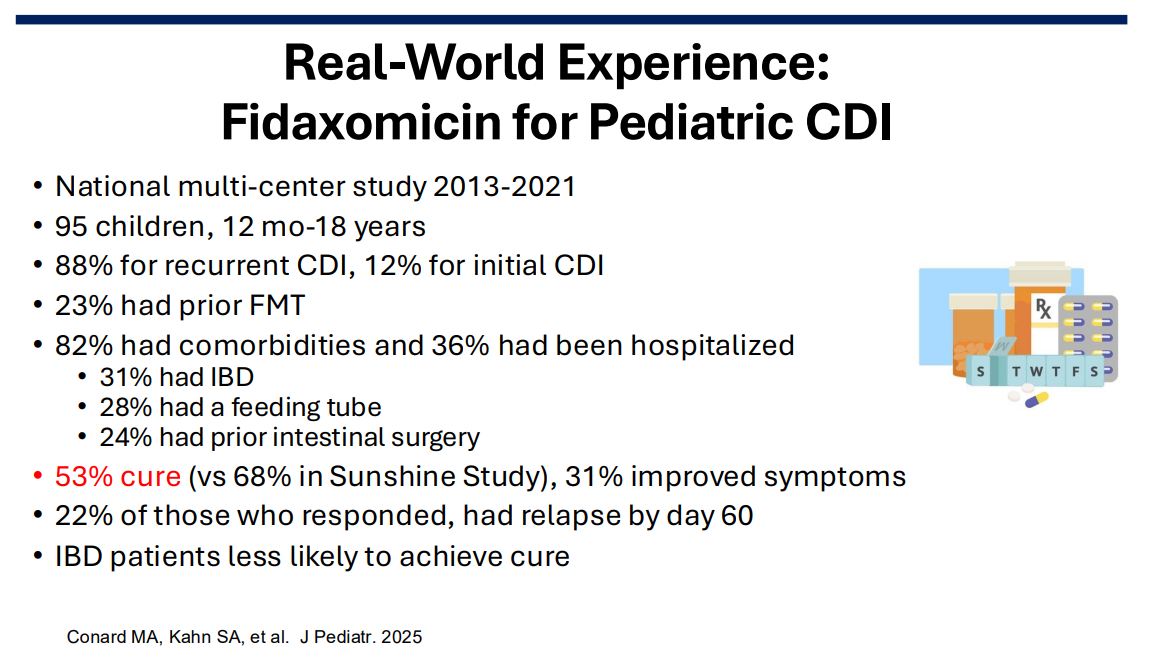
- In patients with IBD who develop an initial episode of CDI, clinicians should preferentially use fidaxomicin or use vancomycin if fidaxomicin is unavailable or cost-prohibitive. Metronidazole should not be used.
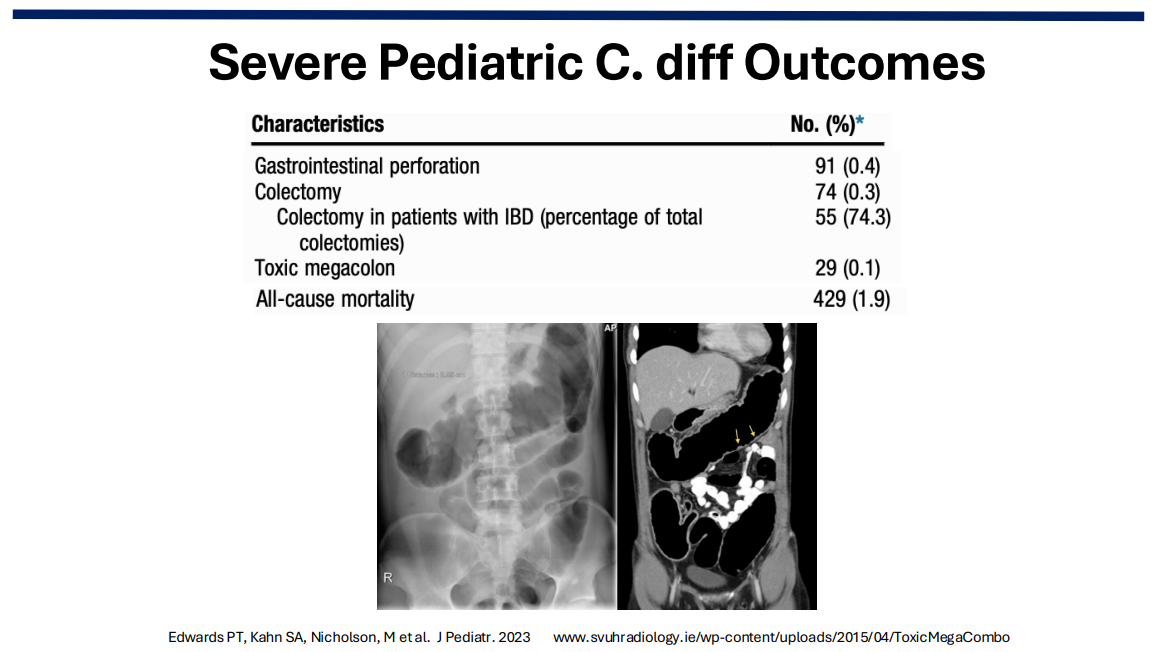
- Clinicians should strongly consider hospitalization for patients with IBD and CDI who demonstrate features of severe colitis or systemic toxicity (eg, more than 6 bowel movements per day, severe abdominal pain, marked leukocytosis, hemodynamic instability, or other evidence of sepsis).
- When selecting an immunosuppressive therapy to treat IBD, no class or mechanism of action has a differential risk of CDI and, therefore, clinicians should choose the therapy that is best to treat the IBD.
- In patients with IBD and acute CDI, concurrent treatment of IBD is critical and clinicians should continue therapy with the required immunosuppressive therapies (ie, immunomodulators, biologics, or small molecules). Steroids can also be used if deemed necessary while CDI is treated with antibiotics.
- Clinicians should consider endoscopic evaluation for IBD activity and exclusion of concomitant cytomegalovirus infection if symptoms persist 48–72 hours after initiation of treatment for CDI.
- Clinicians may consider loperamide in patients with improving inflammation and infection but ongoing diarrhea.
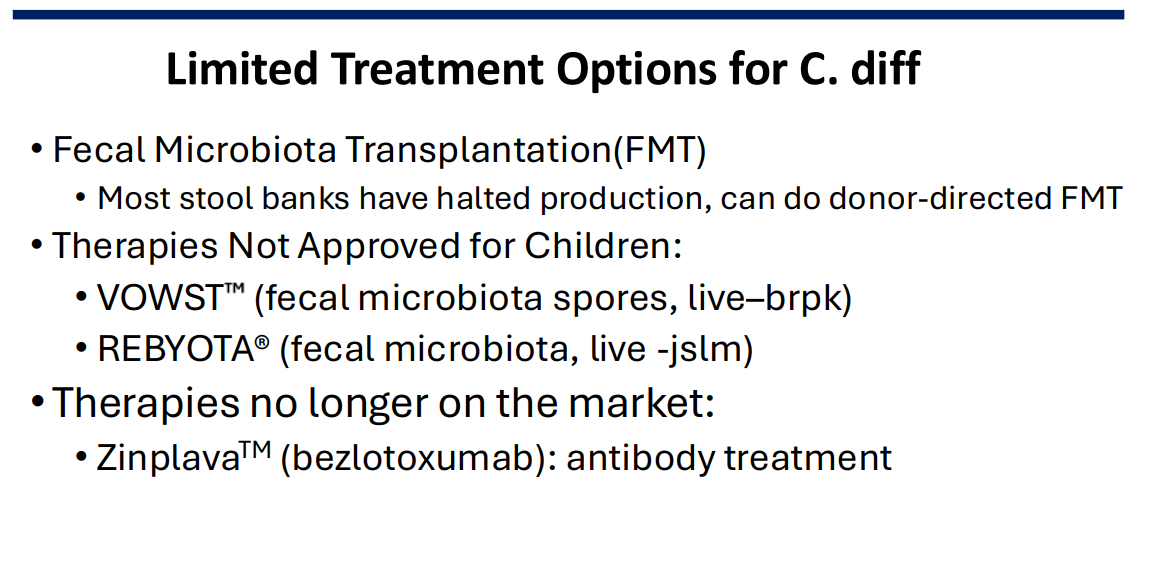
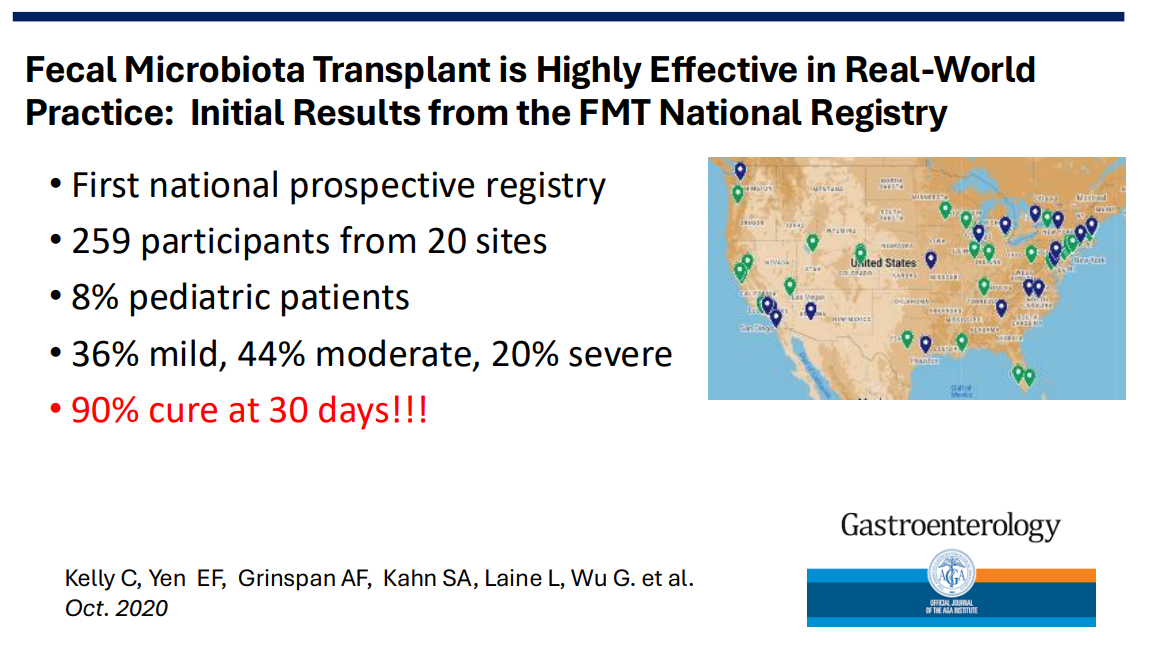
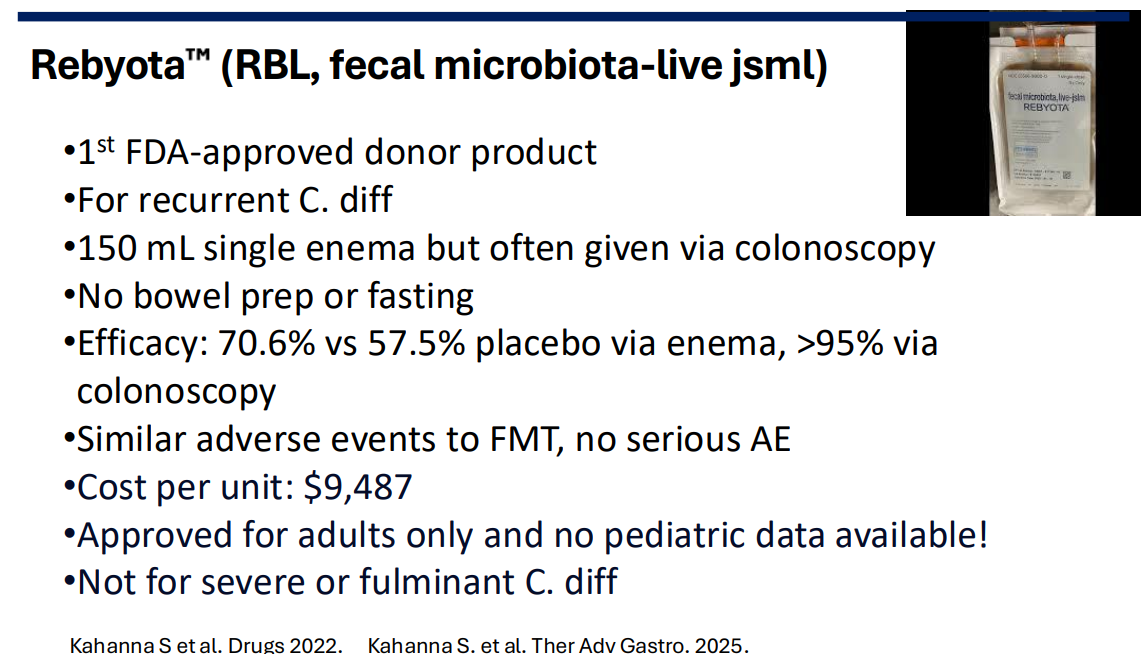
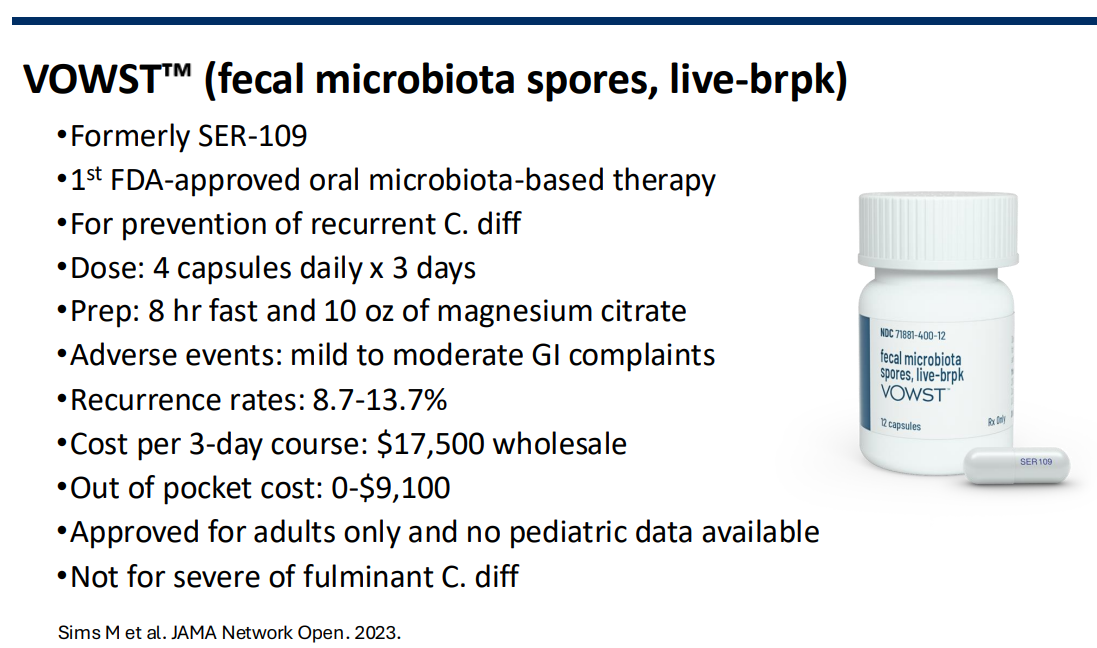
- Clinicians should offer microbiome-based therapies (eg, fecal microbiota, live-jslm, fecal microbiota spores, live-brpk, or unapproved fecal microbiota transplantation) to patients with IBD with at least 1 recurrence of CDI to prevent future infection.
- In patients with IBD, clinicians should not advise probiotics for primary or secondary prevention of CDI.
- In patients with IBD and a history of CDI who are receiving systemic antibiotics, clinicians may consider oral vancomycin prophylaxis as secondary prevention.
Testing Caveats:
- “Because NAAT (nucleic acid amplification test) alone can detect colonization, positive EIA (enzyme immunoassay) with NAAT confirms diagnosis. Positive NAAT and negative EIA should be interpreted with caution due to low sensitivity of EIA.”

Related blog posts:
- Dr. Stacy Kahn: Clostridioides difficile 2026
- Clostridioides difficile Treatment in 2026
- Fidaxomicin Treatment of Clostridioides difficile in Children and Adolescents
- C difficile three-fer: Overdiagnosis with Multiplex Testing, Fidaxomicin Pediatric Approval, & Changing Incidence
- Clostridium difficile and Inflammatory Bowel Disease
- NY Times: “Should We Bank Our Own Stool?” | gutsandgrowth
- Expert Advice on Clostridium difficile and Inflammatory Bowel Disease | gutsandgrowth
- 4 Points for C diff in Inflammatory Bowel Disease
- “Diagnostic Stewardship” –Reducing Unnecessary Clostridioides difficile Treatment by Changing Testing Approach (2024)
- OpenBiome Suspending FMT Shipments (2024)
- ACG Clostridium Difficile Guidelines Plus One (2021)