T Braun et al. Gastroenterol 2026; 170: 971-984. Open Access! Perturbations of Diet and Gut Signatures Persist During Remission in Crohn’s Disease Despite Effective Immune Suppression
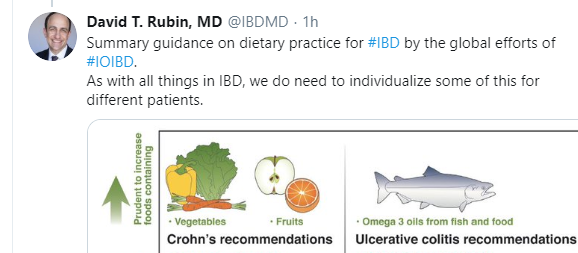
Methods: The authors analyzed diet, ileal transcriptomics, microbiomics, and metabolomics across patients with CD in remission, patients with active CD, and non–inflammatory bowel disease (IBD) controls as the reference for healthy signals.
Key findings:
- Immune signals: Ileal transcriptomics revealed a significant decrease in genes and pathways associated with adaptive T cells and innate granulocytes during remission, which was even deeper than observed in non-IBD controls.
- Antimicrobial gene expression: Patients in remission showed an increase in the expression of epithelial antimicrobial pathways and related genes, including DUOX2, along with an increase in genes associated with goblet cells and mucin glycosylation.
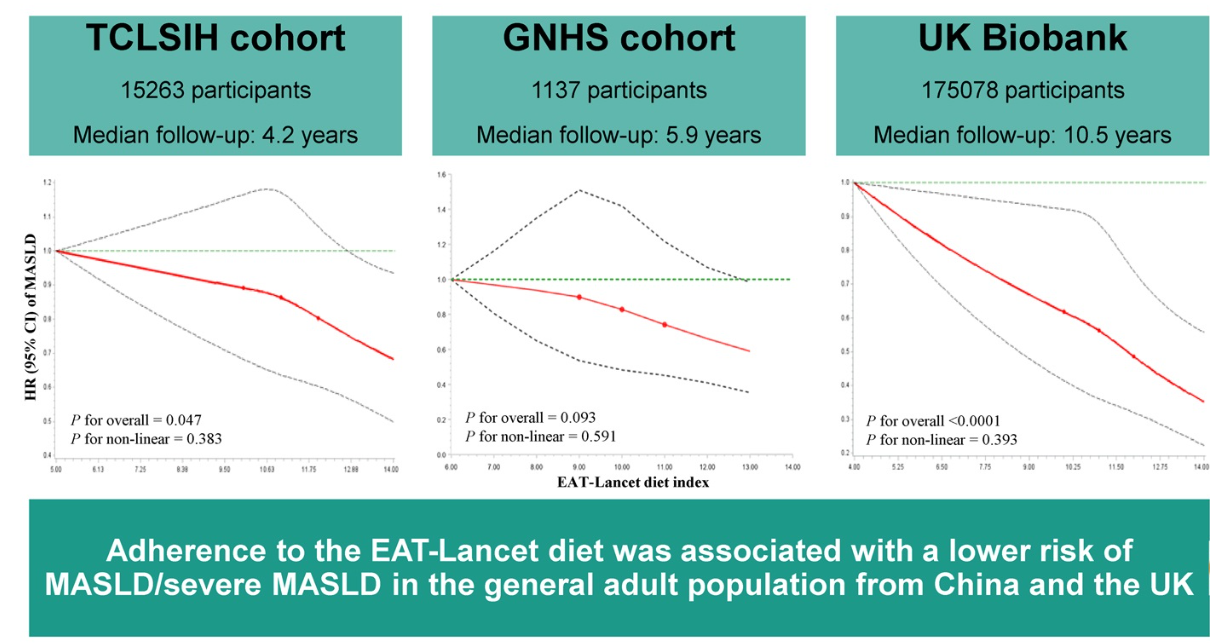
- Microbiome and diet: In patients in remission, there was persistent pathogenic gut microbial composition, metabolic alterations, and less healthy dietary habits, which were characterized by a higher intake of ultraprocessed foods and lower consumption of fiber, folate, vitamin C, and vegetables

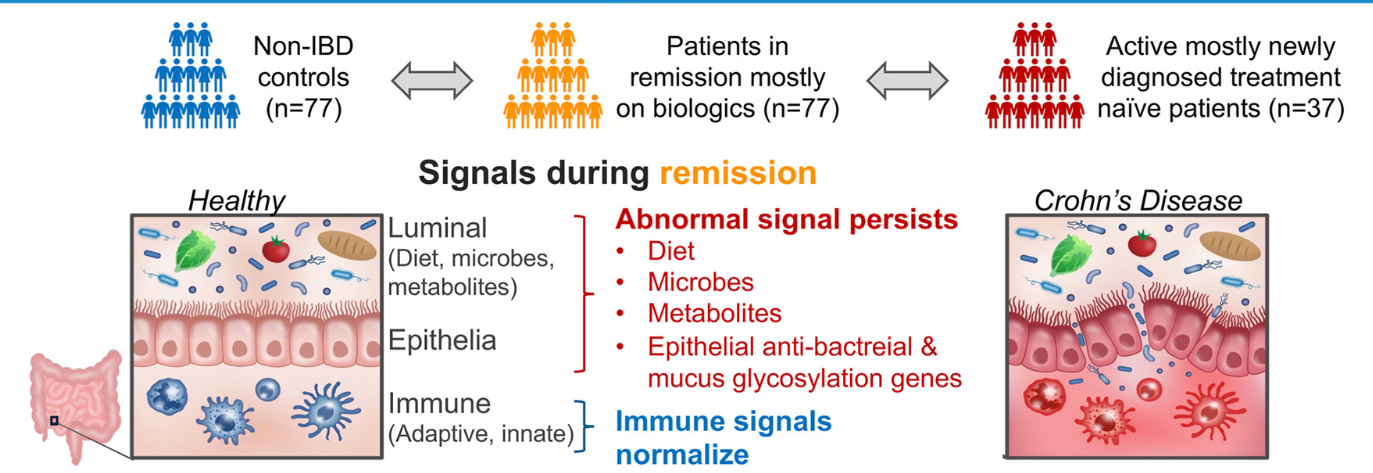
Fecal signals persist during remission and substantially correlate with dietary exposures. (A) Boxplots of Faith’s phylogenetic alpha diversity, our previously defined health index,23 the previously defined Gevers IBD dysbiosis index21, and our IBD-specific index23 between controls, CD patients in remission, and CD with active disease.
My take (borrowed from the authors): This study shows that, during remission with advanced therapies, “disturbances in antibacterial epithelial signals, along with unhealthy dietary patterns, altered microbiome, and perturbed metabolome, continue and are partly linked to the risk of flare 6 months later.”
Related blog posts:
- “Tasty & Healthy” Whole Food Diet For Crohn’s Disease
- Mediterranean Diet’s Impact on Crohn’s Disease Outcomes
- Mom, Can We Get a Dog (& a Sibling)? I Don’t Want to Get Crohn’s Disease
- Risk Factors for Inflammatory Bowel Disease: Ultra-Processed Food (Part 1)
- Ultraprocessed Food and the Risk of Inflammatory Bowel Disease