
More from Aspen Webinars. This blog entry has abbreviated/summarized several presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
Dr. Mieli-Vergani presented case report of a boy with autoimmune sclerosing cholangitis and associated colitis who presented with minimal symptoms.
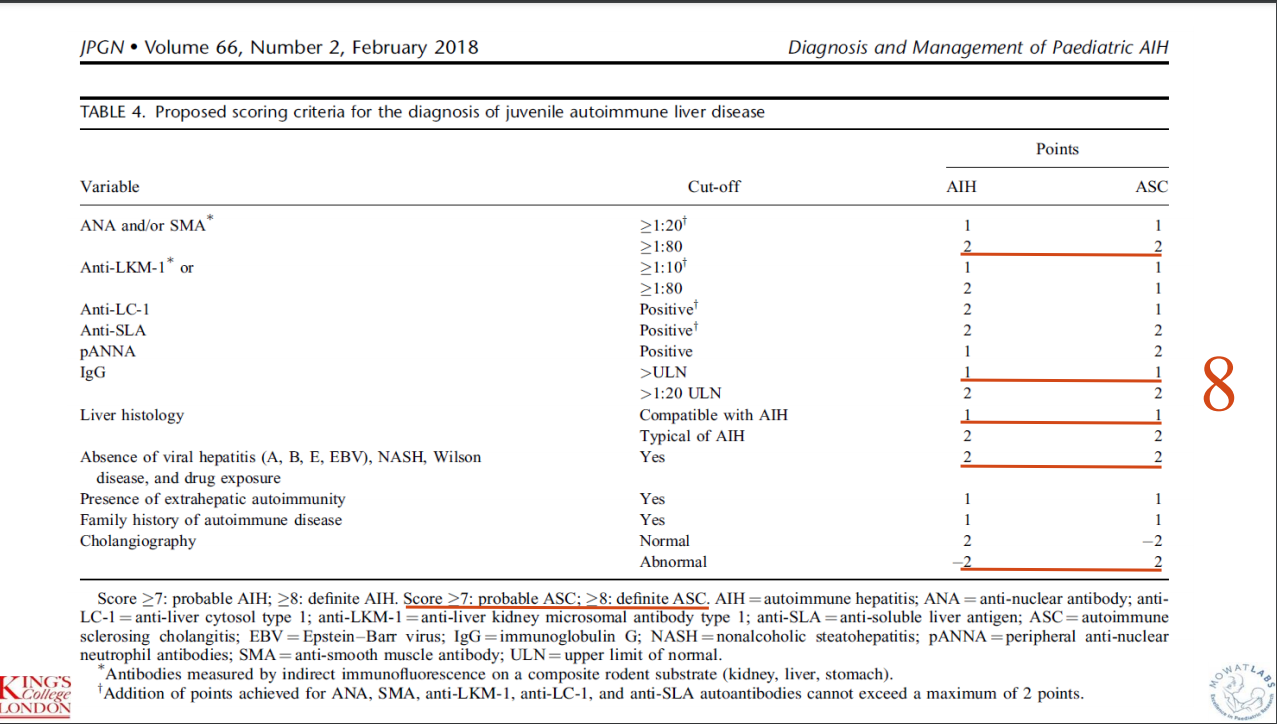
This case report highlights the evaluation and management of autoimmune liver disease hepatitis. Workup included autoimmune serology, GGT, celiac serology, calprotectin, and ultrasonography. EGD-Colonoscopy was prompted by elevated calprotectin. MRCP was prompted by elevated GGT (GGT were normal at the time of biopsy and MRCP) and liver biopsy findings.
“My message is that MRCP and colonoscopy should be done in all cases of autoimmune liver disease in children and adolescents, irrespective of calprotectin levels or elevated GGT and biliary changes on histology, as both IBD and sclerosing cholangitis can be present without any of the classical symptoms and signs. Only by doing this it is possible to reach an early diagnosis which is essential for early treatment and for a good outcome.”
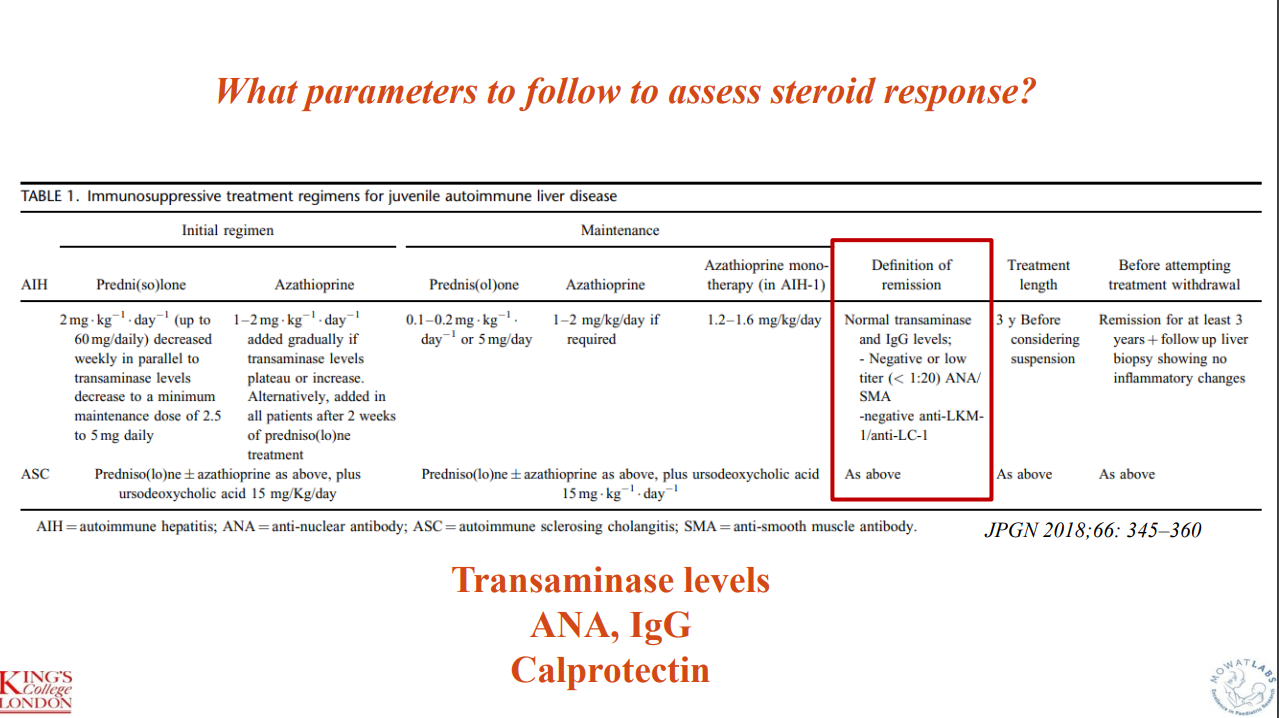
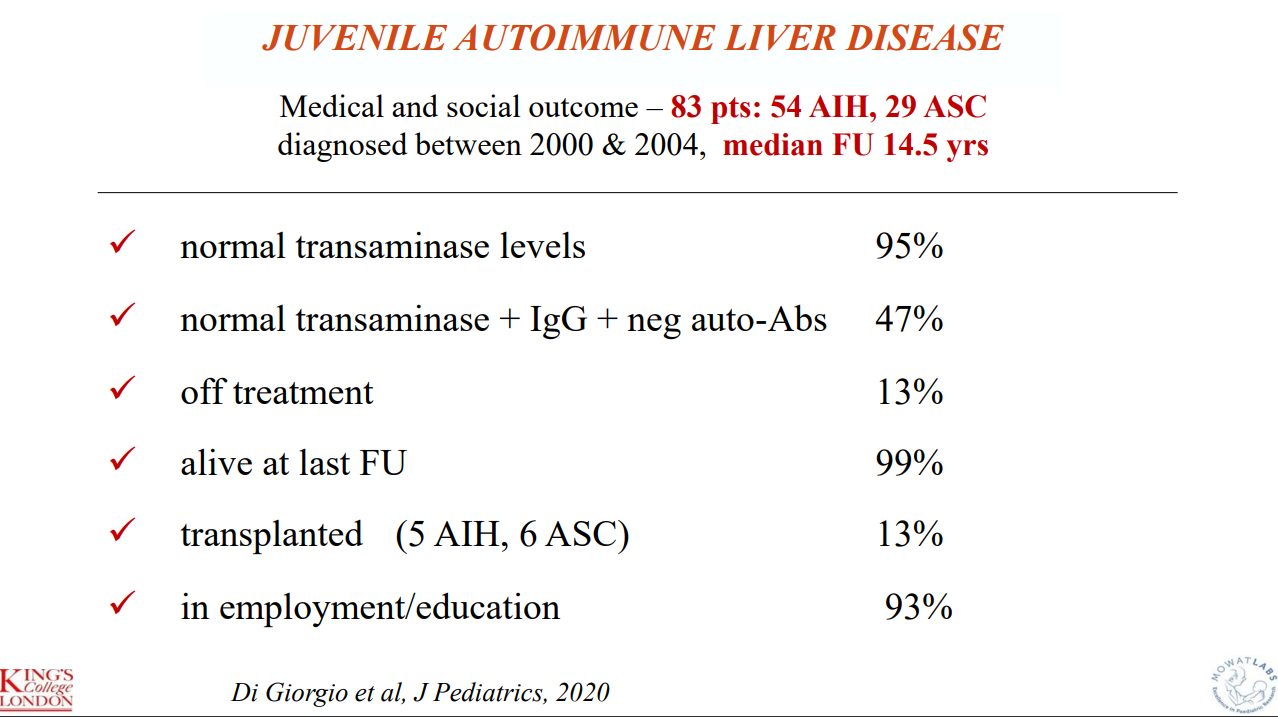
Outcome data indicate that 11 of 83 (13%, 5 AIH, 6 ASC)) required transplantation. “I have shown our long-term outcome data not to stress the number of patients who have required transplantation, but the number of patients who are well and have a normal life after over 14 years of follow-up. This can be only achieved if one thinks of autoimmune liver disease even if the child appears to have something non-specific, initiating correct treatment for the liver, and the gut if there is bowel disease, as soon as possible. At the beginning, treatment should be monitored very closely (at least weekly), to be able to decrease the dose of steroids swiftly, introduce azathioprine if needed, and avoid side affects.”
Key points:
- Budesonide is not a good substitute for prednisone in autoimmune hepatitis
- Mycophenolate is frequently used as a 2nd line agent
- Consider calprotectin in patients with autoimmune liver disease to screen for IBD (though calprotectin can be falsely-negative)
- Consider followup liver biopsy after normalization of liver enzymes for ~3 yrs (when consideration of stopping medications)
- Recommends MRCP for all patients with AIH
Some slides:
Key points:
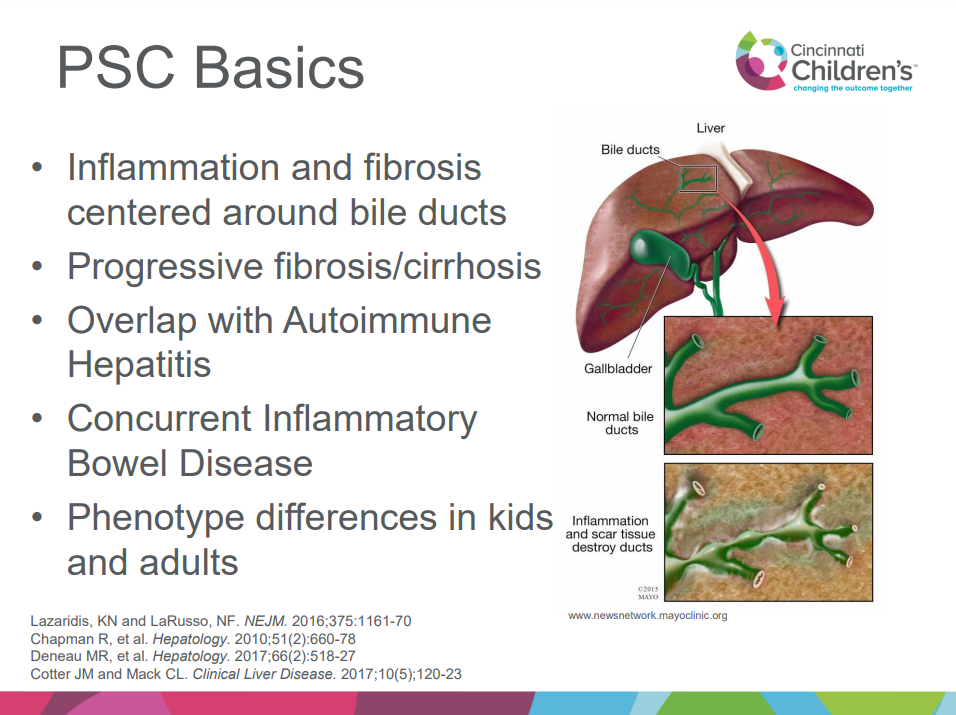
- Better understanding of immune basis of PSC is developing
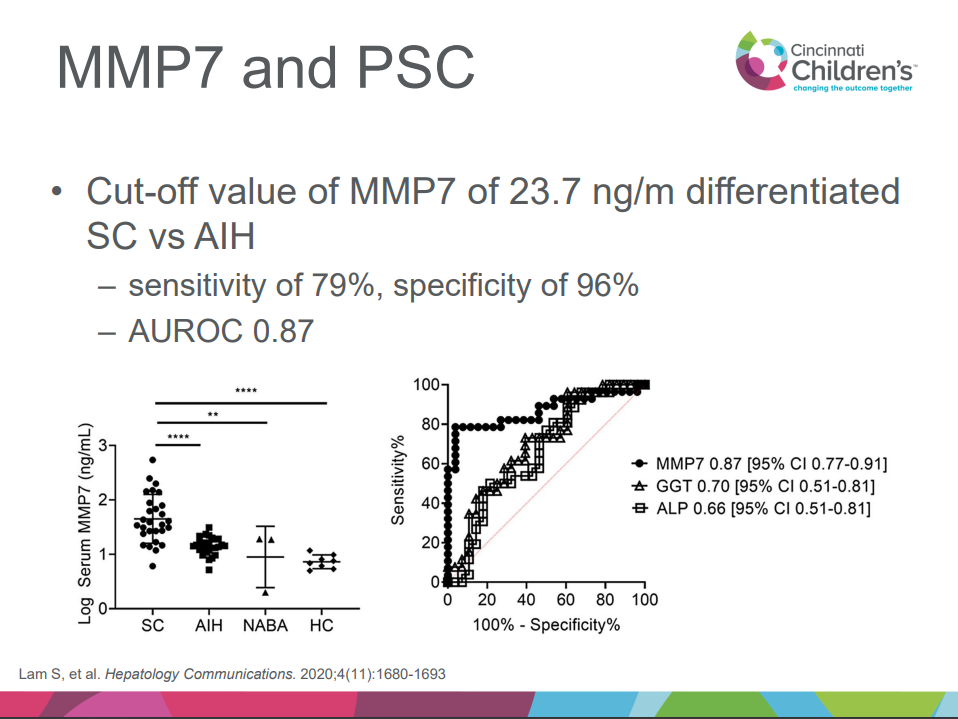
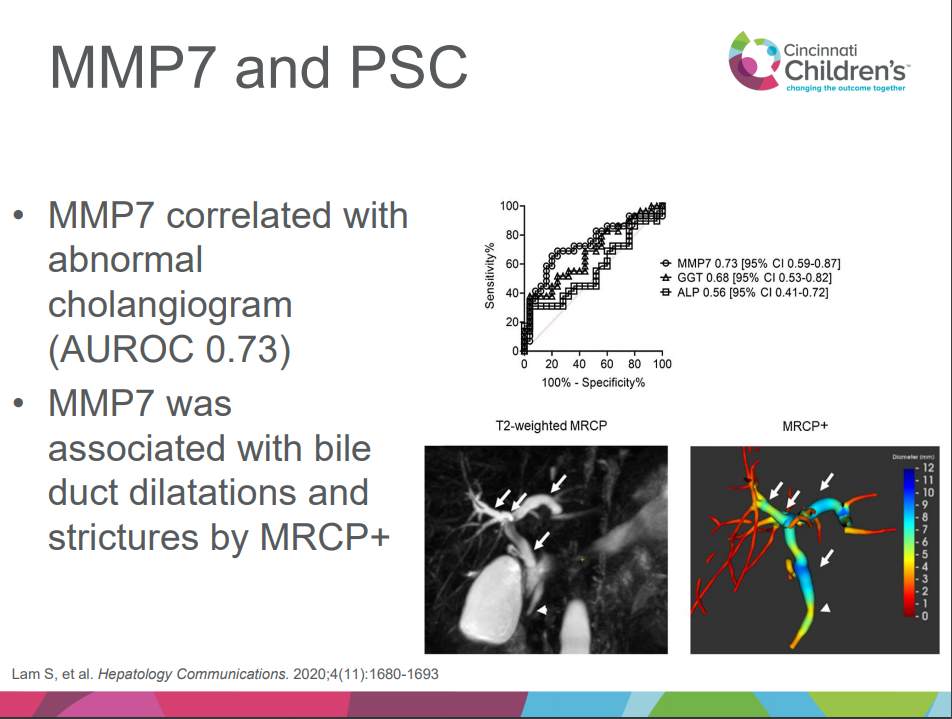
- MMP-7 appears to help differentiate PSC/ASC from AIH
- Small duct PSC is more common in children
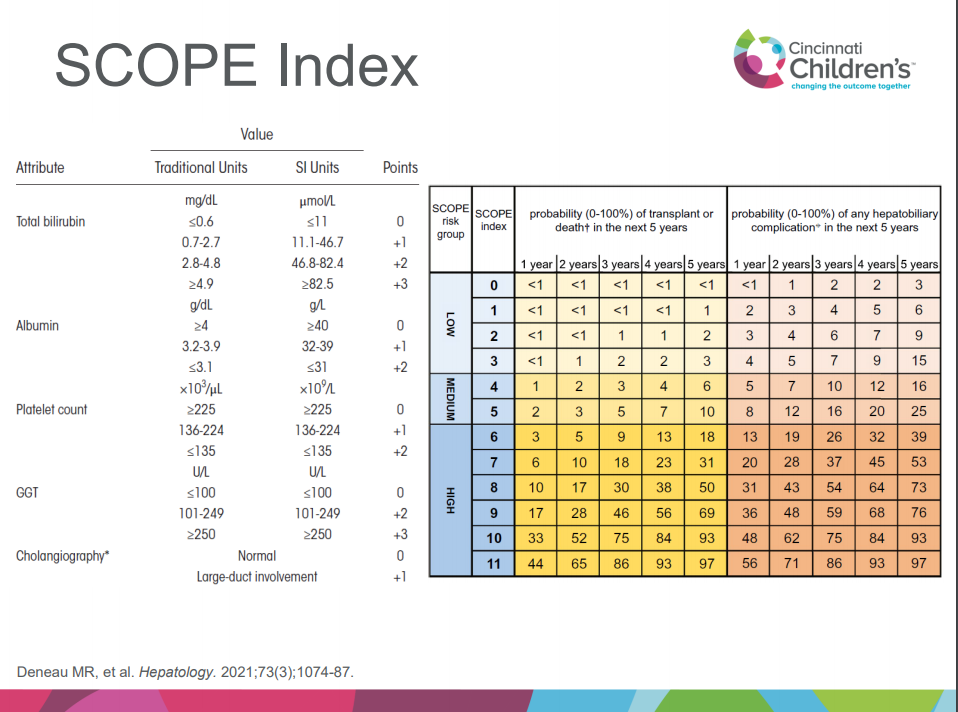
- SCOPE index can help predict outcomes
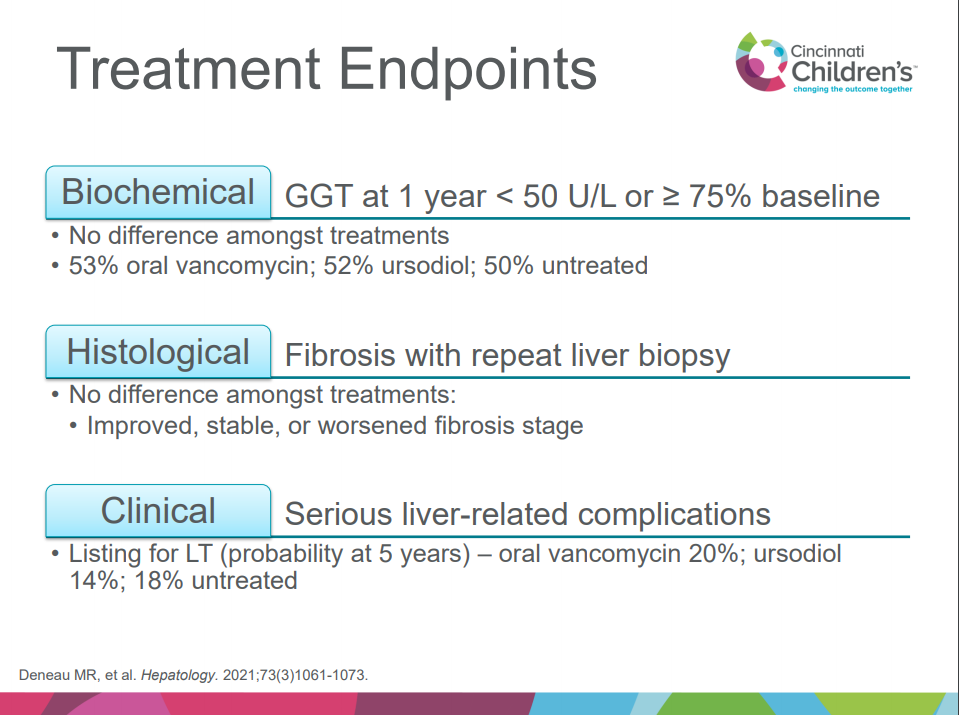
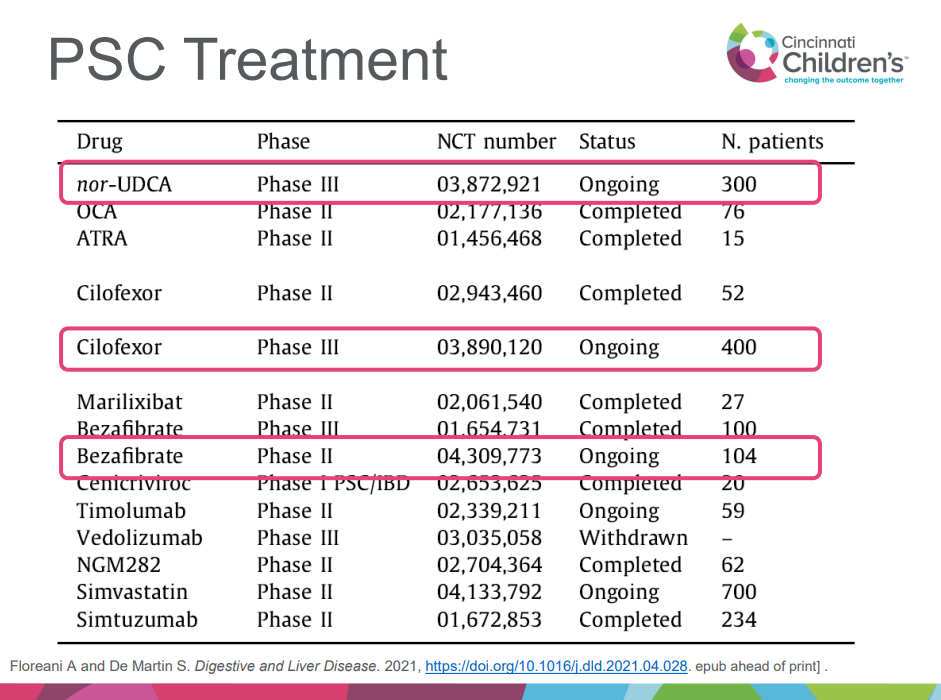
- Treatment: no clear benefit of vancomycin, ursodeoxycholic acid compared to placebo but need for randomized controlled study
- Several studies of new agents for PSC in adults are ongoing, including nor-UDCA, cilofexor, bezafibrate
- Vedolizumab does not appear to be effective for PSC
- Related blog post: Online Aspen Webinar (Part 3) -2020 lots of links to other related blog posts
Some of the slides:
Milo Rezvani -case report
Child with FTT, elevated LFTs, sporadic mild hypoglycemia, and neurologic symptoms. DDx: congenital disorders of glycosylation (CDG), mitochondrial d/o, peroxisomal d/o, urea cycle d/o and lysosomal d/o. Diagnosis was made after liver biopsy and whole exome sequencing (which showed PMM2 mutations). Diagnosis of most CDG can be made by serum transferrin isoforms. Discussion among many participants noted that liver biopsy often not needed in age of genetic testing.

Pingback: Recurrent PSC in Children After Liver Transplantation | gutsandgrowth
Pingback: Long-Term Outcomes of Pediatric Patients with Sclerosing Cholangitis in the Setting of Inflammatory Bowel Disease | gutsandgrowth