
A recent review (Full text: LJ Saubermann et al. JPGN 2017; 64: 639-52) discusses the hepatic issues and complications associated with inflammatory bowel disease.
Key topics:
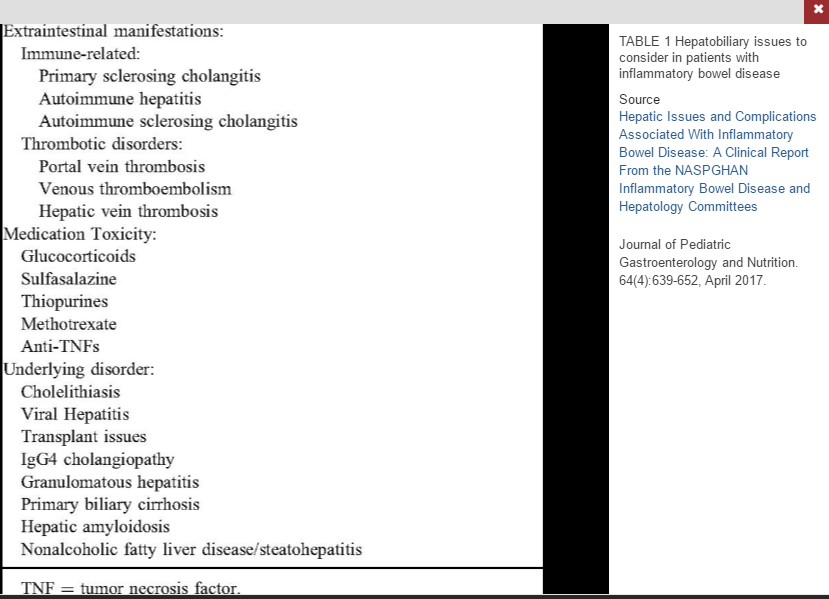
- Primary Sclerosing Cholangitis (PSC)
- Autoimmune Hepatitis (AIH)
- Autoimmune Sclerosing Cholangitis (ASC)
- Portal Venous Thrombosis/hypercoagulability
- Cholelithiasis (more common in Crohn’s disease if diseased terminal ileum)
- Viral hepatitis
- Drug-Induced Liver Disease
- Fatty Liver disease
Many of these topics have been discussed previously on this blog. A couple of pointers in this review:
PSC:
- Greater risk of colorectal carcinoma
- IBD-PSC patients are at higher risk for pouchitis
- GGT of >252 U/L “was highly sensitive (99%) and had good specificity (71%) for PSC” [or ASC]
- The authors recommend “screening all newly diagnosed patients with IBD with ALT and GGT
- Immunosuppressive therapy is NOT effective
- Vancomycin therapy is currently being tested (clinical trials: NCT02137668 & NCT01802073)
AIH:
- Less frequent in IBD patients than PSC
- Most common treatment is prednisone/azathioprine
- 40-80% of children have cirrhosis at AIH diagnosis, but “progression to end-stage liver disease is rare and …with appropriate treatment, 80% of patients achieve remission.”
ASC:
- ASC is an overlap syndrome between AIH and PSC
- “It is important that children with IBD and apparent AIH are routinely investigated for evidence of biliary disease with MRCP”
- “ASC responds to the same immunosuppressive combination therapy used for AIH”
HAV/HBV Immunization:
- HAV vaccination is effective in patients with IBD…although the rate [seroconversion] was significantly lower” in patients receiving anti-TNF therapy (92.4% vs 99.1% in one study).
- In those needing HBV immunization: “One strategy evaluated to improve HBV immunity in adults with IBD is an accelerated course with double vaccine doses at 0, 1, and 2 months.”
Methotrexate (MTX):
- “The extent of histological features of hepatotoxicity secondary to long-term MTX use in IBD has been infrequently described; however, the inicdence of significant abnormal histological findings appears to be rather low.”
My take: This article is a good starting point for liver-related issues in IBD. For concerns regarding medications, the NIH livertox website is more useful and much more comprehensive.
Related blog entries:
DILI:
PSC:
- Population-Based Outcomes for Primary Sclerosing Cholangitis
- Should we care about subclinical PSC?
- Screening for subclinical PSC in IBD? | gutsandgrowth
- Vedolizumab for Primary Sclerosing Cholangitis (with … – gutsandgrowth
- Population-based outcomes for PSC gutsandgrowth
AIH:
- Withdrawing Immunosuppression with Autoimmune Hepatitis
- Diagnosing Autoimmune Hepatitis
- Adult versus Pediatric Data for Autoimmune Hepatitis

Pingback: More IBD Cases Than Ever in Young Canadian Children | gutsandgrowth
Pingback: Steroid-Free Approach in Autoimmune Hepatitis | gutsandgrowth