
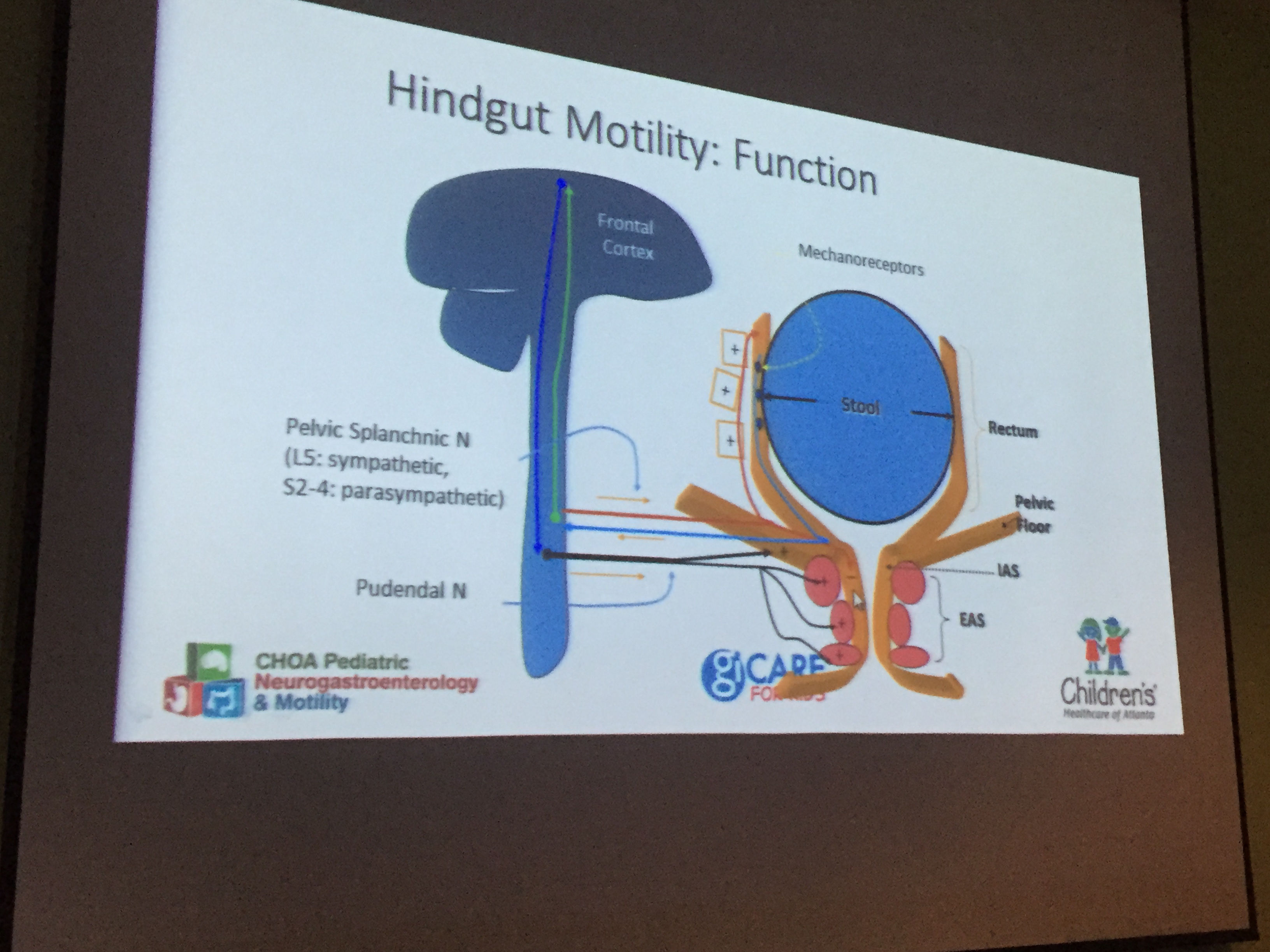
Recently I attended a terrific talk by my partner, Jose Garza. This lecture provided a great deal of information on refractory constipation for both pediatricians and pediatric gastroenterologists alike.
Elements of the talk included diagnosis, pathophysiology and differential diagnosis.

Rome III Criteria -Helpful in Diagnosis of Constipation

Is it Hirschsprung’s Disease?
Some of the more useful points.
- AXR should not be used to make diagnosis of constipation.
- Many refractory constipation patients are stooling fine and actually labeled as constipation instead of a functional abdominal pain disorder. That is, they are complaining of stomach pain and have been erroneously told they are constipated (see point #1).
- Miralax remains a 1st line agent for constipation. In individuals with fecal soiling, if miralax is not working and they have had appropriate cleanout, then senna laxative may be helpful.
- Sitz markers are particularly helpful in proving stooling when teenager claims to not be stooling for a month and in proving functional fecal retention rather than nonretentive soiling.
- If good treatment is not working, then refer to neurogastroenterology.
Related blog posts:
- What’s Wrong with Ordering an AXR for Constipation in the …
- Miralax -More Scrutiny, Research Study | gutsandgrowth
- It’s worth the cost | gutsandgrowth
- AGA Constipation Guidelines | gutsandgrowth
- Miralax Safety – gutsandgrowth – WordPress.com


Pingback: Soiling Stinks! | gutsandgrowth
Pingback: Rectal Suction Biopsies Less Accurate in Infants <40 days | gutsandgrowth
Pingback: Do You Know the Best Way to Use Antegrade Enemas? | gutsandgrowth
Pingback: More than Two Years of Constipation Before Specialty Help | gutsandgrowth
Pingback: Safety of Senna-Based Laxatives | gutsandgrowth
Pingback: New Data on Bisacodyl for Pediatric Constipation | gutsandgrowth