
Earlier in the year, I summarized the upcoming changes for 2021: Link Get Ready for 2021 Coding Changes (with links to AMA resources and tables). Subsequently, I went to a coding seminar led by Jan Rasmusen and wanted to share some additional observations.
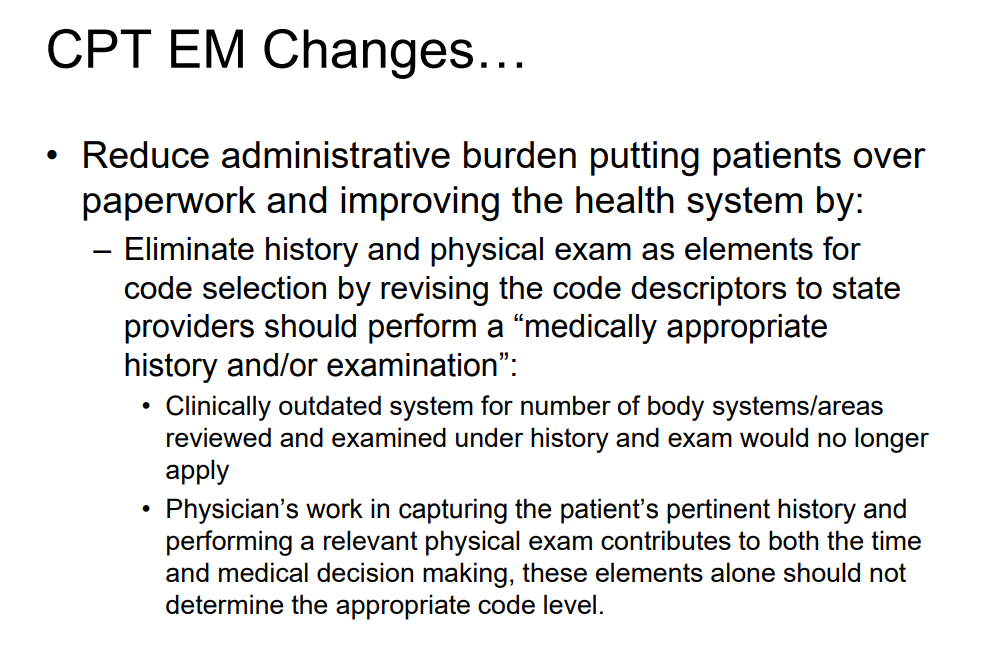
- One of the most important changes is the need for “medically appropriate history and/or examination” rather than focusing on specific elements. This helps eliminate scoring the history and physical exam and should allow more time to document critical thinking. Besides billing, H&P is still key for helping with continuity of care and for liability.
2. When using time codes and not using medical decision-making, the total time –face-to-face and non face-to-face –is what is used. Total time does not include clinical staff time.


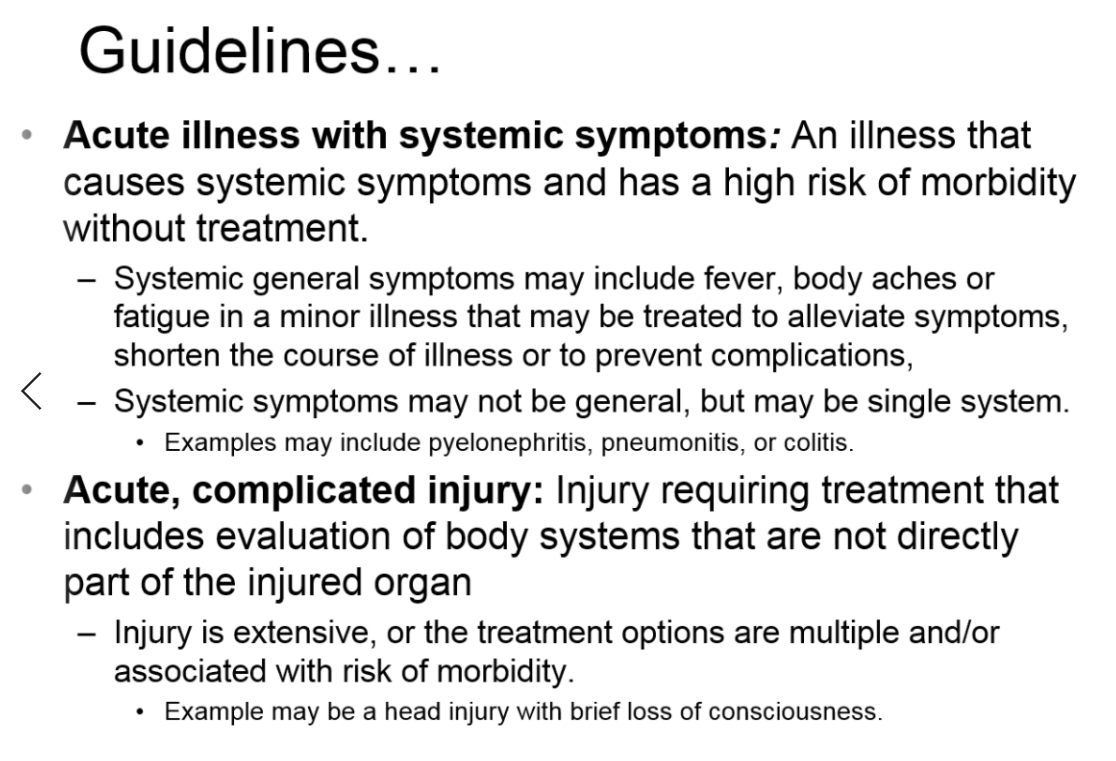
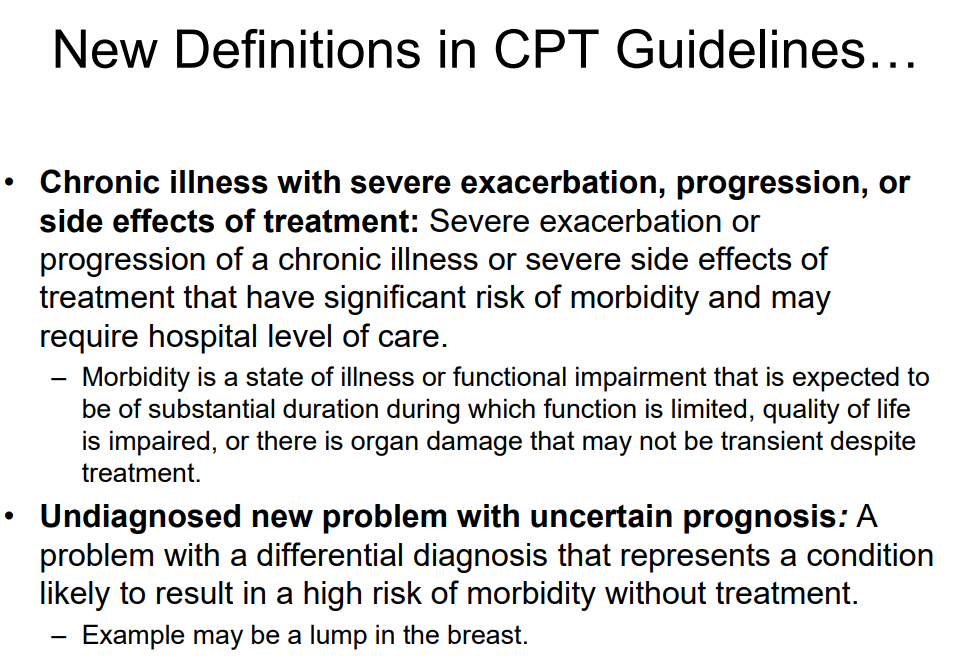
3. A lot of the terms have more specific definitions


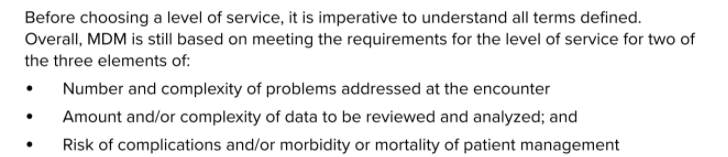
4. Medical Decision-Making is Similar to Current Guidelines

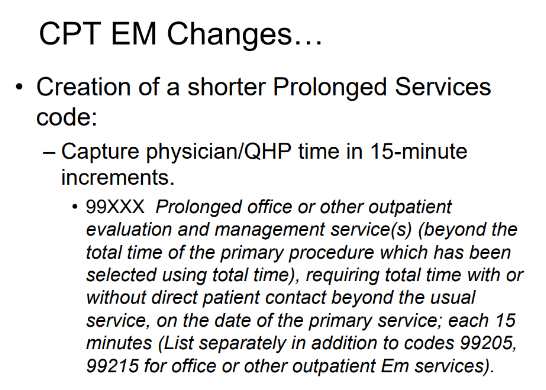
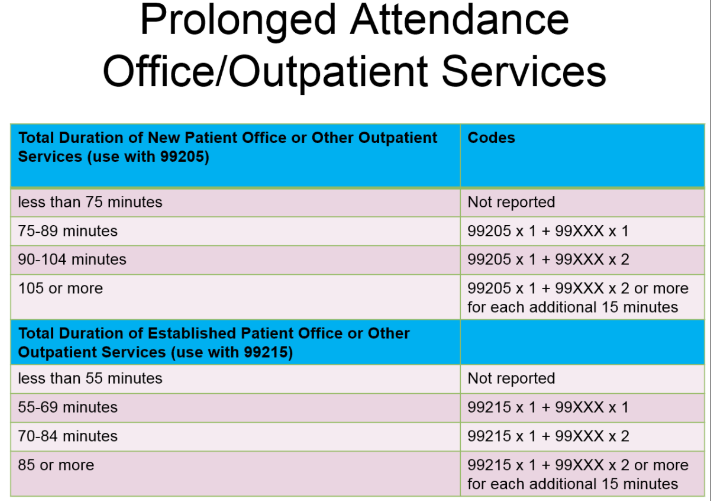
5. Creation of a new code for additional time
My take: The intent of these changes is logical. The goal of coding is to align the reimbursement with the degree of effort and not simply allow pre-formatted templates to justify upcoding. These changes could lead to simplification of documentation and allow more documentation time for medical decision-making part of the visit.
Resources:
- 2021 E/M changes: https://www.ama-assn.org/system/files/2019-06/cpt-office-prolonged-svs-code-changes.pdf
- AMA E/M learning module: https://edhub.ama-assn.org/interactive/18057429
- AMA MDM table (see below): https://www.ama-assn.org/system/files/2019-06/cpt-revised-mdm-grid.pdf
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition

Is there any guidelines or anything developed to use for Pediatric GI, like Crohn new patient would typically fall into level 5 or Celiac follow-up would fall into level 3?
I have not seen specific Pediatric GI guidance. Based on medical complexity, many new IBD patients could qualify at highest level as could short bowel patients. Celiac followup complexity would depend in part on how they are doing, if there are associated problems, and amount of data that needed to be reviewed.