
D Blumenthal et al; NEJM 2024; DOI: 10.1056/NEJMp241085. The Failing U.S. Health System
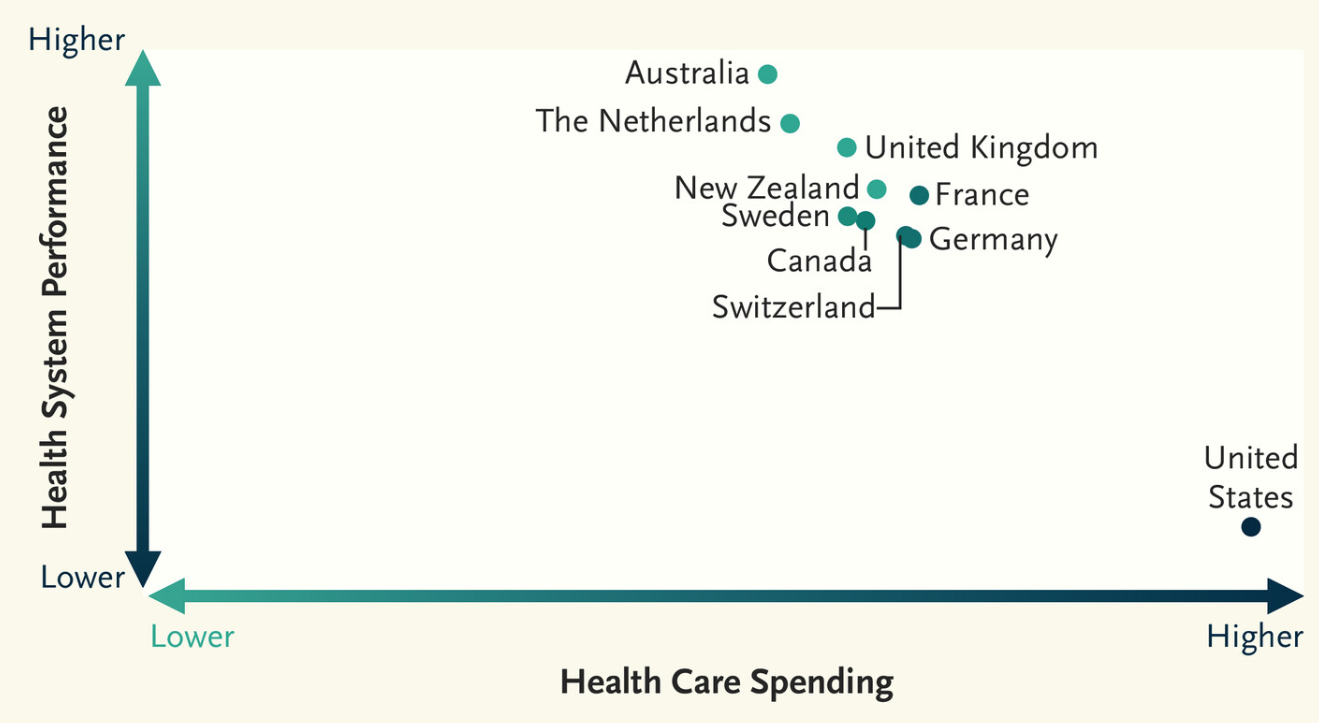
This article succinctly explains why the U.S. health system spends a lot and has the worst performance of similar countries.
Some excerpts:
- “In Mirror, Mirror 2024, the Commonwealth Fund’s eighth report since 2004 comparing the health systems of 10 high-income countries…The United States has the lowest life expectancy among the 10 countries we studied, 4 years less than the 10-country average.”
- “It also ranks last on measures of preventable mortality and “treatable mortality”…These measures capture deaths that could have been averted by means of preventive services or timely and effective treatment, such as deaths from hypertension, diabetes, cerebrovascular disease, ischemic heart disease, or renal failure. The United States had the highest excess mortality attributable to Covid-19 among people younger than 75 years of age in 2021. It also has the highest rate among the 10 countries of death from self-harm, which includes deaths by suicide, and the highest rate — by orders of magnitude — of death from assault, which includes deaths caused by gun violence.”
- “The United States ranks last on measures of access to care and equity of care…Another contributor to access barriers is inadequate coverage among insured Americans because of high deductibles and copayments.”
- ” The Affordable Care Act and related policies reduced the proportion of uninsured people to its current level of 7 to 8%. But 26 million Americans still lack insurance.”
- “Providing insurance, however, will not be sufficient. The U.S. health care delivery system has profound problems … One such problem is the country’s worsening shortage of primary care clinicians”
- ” the high prices charged by U.S. health care facilities and professionals, which far exceed prices in other health systems.3 … One of the reasons health care organizations are able to charge such high prices is that they have obtained increasing economic power in local markets as a result of consolidation — both horizontal consolidation among hospitals and vertical consolidation, which involves large organizations acquiring physician practices. The arrival of private equity investors who “roll up” physician practices in local markets and then raise prices has also contributed to the escalation of U.S. health care costs.4“
- “The United States lags behind comparator countries when it comes to addressing the social determinants of health, such as poverty, homelessness, inequality, and hunger.”
My take (borrowed from authors): “What is the future of a country that allows an untold number of its people to suffer and die unnecessarily because of a lack of access to basic health services, inadequate public health measures, and a tattered social safety net?”
Related blog posts:
- “More Than Half a Million Extra Deaths” Every Year In U.S.
- NY Times: America can afford a world-class health system. Why don’t we have one? | gutsandgrowth
- Life Expectancy Dropping in U.S.
- What Is Driving Hospitals’ Acqui$ition of Physician Practices?
- “Health Insurance Is Broken” | gutsandgrowth
- When Hospitals Look Like The Ritz (But Cost Even More)
- “America’s Huge Health Care Problem” | gutsandgrowth
- “Do Nonprofit Hospitals Deserve Their Tax Exemption?”
- Healthcare: “Where the Frauds Are Legal”
- Medical Billing Trap: Hospital Pricing for Urgent Care Visits and Outpatient Departments
- NPR: Drugmakers Claim to Lose Money in US In Order to Avoid Taxes
- Heroes, Villains and ‘Perverse’ Incentives. Story of Big Hospitals vs. Big Pharma | gutsandgrowth
- Worse Outcomes After Hospital Mergers | gutsandgrowth

Unable to access the complete article, it appears that many valid points are made. While ACA may have brought the uninsured level to 7-8% (previously 16%), it also helped promote the massive amount of consolidation. As healthcare providers (and maybe non-providers), I think we would agree that all too often consolidation has not helped the system and led to major cost of care issues.
Additionally, there is an underlying culture in American healthcare that puts the burden of care completely on the provider. “Will your office be calling me to schedule my follow-up” and many other examples of this exist. This I believe is more prevalent and unique to the American healthcare system/American culture. We need to expect more from our patients and put more of their care on their shoulders.
Similar issue with link and paywall on the article. But, as someone who has lived 5 years and participated in the Swiss medical system, there are some profound differences and similarities to learn from.
-Most of the state systems in Europe occurred after WWII–out of necessity because there was no private system, and they never switched back. Switzerland did not have that to deal with after the war and has always been a private system.
-Health insurance is sold to individuals—employers CANNOT be involved—and the government sets the minimum standard of insurance. Insurance companies are authorized to sell their product but can only base their rate on age and whether one smokes. For those that can’t afford it, government assistance helps buy those policies. This is what a free market looks like, not what we have in the US: where one has to practically be an attorney to be able to read the fine print to understand policy differences.
-Having health insurance is a government mandate. One cannot register their kids in school or collect a paycheck from their employer without proof of health insurance. I was able to experience that directly.
-A doctor is a normal career that starts with someone going to school (to be a doctor) and immediately thereafter being employed as a junior doctor at a hospital, with a professional salary starting in their 20s. The current US educational system for physicians requires a decade-long investment in higher education that is unnecessary. It’s a pyramid scheme. In Switzerland, higher education is paid for, but the number of paid slots for various professions are set by the government. Higher education funding is a targeted investment in society and future taxpayers, not a blank check to study one’s fancy–as it is in the US.
-It was normal to see about a 1:1 ratio of doctors to office staff in a normal doctor visit—the office staff also doubled duty as nurses typically. One doesn’t need to be an engineer to see that fraction of value-add personnel in US healthcare is small.