
JA Busam, ED Shah. Clin Gastroenterol Hepatol 2026; 24: 281-284. A Decade of Decreasing Reimbursement Strains Gastroenterology Practices and Threatens Their Independence
Background: “Over the past decade, a remarkable number of independent community gastroenterologists became part of larger groups, primarily due to financial concerns. Although the number of gastroenterologists increased between 2012 and 2020, the number of associated practices decreased by more than 650 (14%), with the number of physicians practicing in groups of less than 10 decreasing by nearly 1500 (35%).1 Simultaneously, the number of self-employed physicians decreased,2 while the number of hospital-employed and private equity affiliated physicians increased.3,4 Surveys of practices engaged in such consolidative behavior most often cite financial uncertainty given increased costs, decreased revenues, and continuing regulatory pressures, along with personal financial gains, as important motivations.5,6“
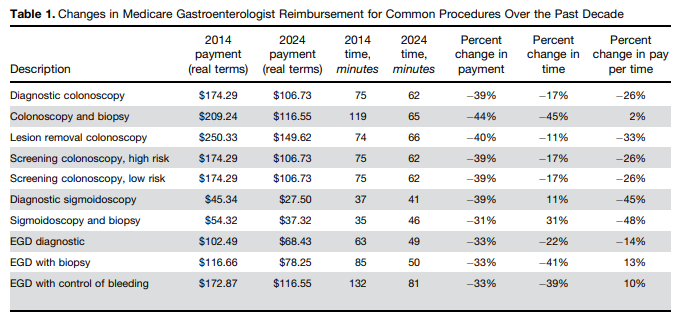
Methods: The authors examine how “Medicare reimbursement has affected independent, community practices over time, with a particular emphasis on hourly rates to account for any efficiencies in endoscopic procedure times over the past decade…[using] multiple datasets from the Centers for Medicare and Medicaid Services (CMS).”
Key finding:
- “All major endoscopic procedures investigated brought in decreased associated professional revenue between 2014 and 2024 per unit billed. Most procedures saw a reduction between 30% and 40% in the amount of cash brought into the practice per procedure”
- “Although independent practices faced tough decisions due to these trends, other health care stakeholders benefited. Concurrently, facility revenues, medical complexity,13 overall health expenditures,14 drug prices,15 and pharmacy benefit manager profits16 all increased, the latter by approximately 80%”
My take: This small study shows how “independent gastroenterology practice reimbursement decreased substantially since 2014 despite increasing patient complexity and capital flows into health care, threatening the viability of many community practices.”
Related blog posts:
- Gastroenterology and the Rise of Private Equity Investments
- Why Corporatization Occurs in Health Care
- Unpacking Health Care Corporatization in the U.S.
- How Much of a Drug Markup is Reasonable (for hospitals)?
- “Commercial Insurance Isn’t in the Health Care Business. It’s in the Financial Business.”
- Exploring Walgreens’ Collapse: The Role of PBMs
- “The Broken Promises of Profit-Driven Medicine”
- ‘Physicians Are Not the Victims’ (Plus One)
