
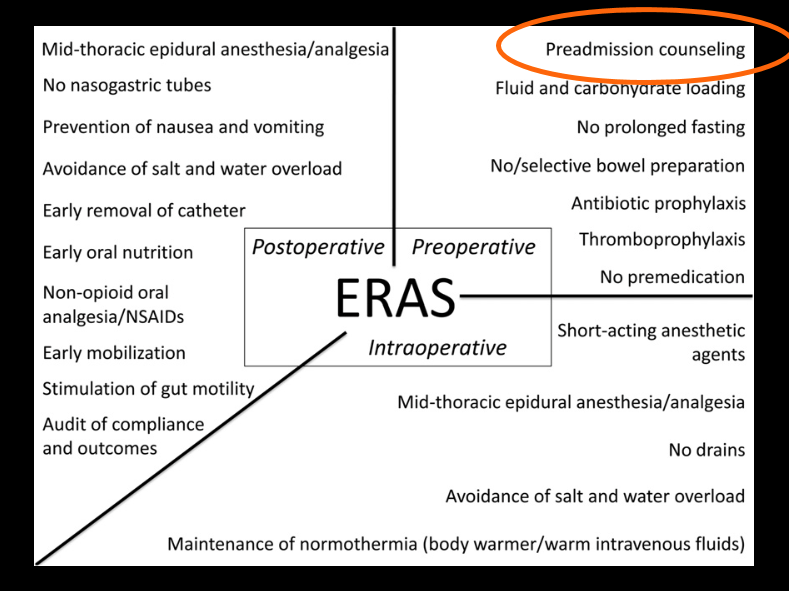
Fortunately, only a small number of children need colorectal surgery. For those who do need this surgery, there are advancements which are helping to reduce length of stay and shorten recovery. Some of the concepts with “Enhanced Recovery After Surgery” or ERAs have been around for more than 10 years. One of our surgical colleagues, Dr. Kurt Heiss, described his experience in applying these techniques in the pediatric population and was kind enough to share his slides. Slide 10 (see below) outlines the key points.
The immediate challenge in improving the quality of surgical care is not discovering new knowledge, but rather how to integrate what we already know into practice –Urbach DR, Baxter NN, BMJ 2005
Preoperative:
- Counseling family
- Avoid bowel prep –>can lead to bowel edema
- Avoid prolonged fast prior to surgery. Fluid/carbohydrate loading
- Use of Neurontin preoperative
- Antibiotic prophylaxis
- Thromboprophylaxis
Intraoperative:
- Short-acting anesthetics
- Use of TAP and/or short-term epidural. Avoid narcotics
- Avoid excessive fluid administration
- No drains
- Maintenance of normothermia
Postoperative:
- Early feeding (same night)
- No NG
- Avoid/minimize narcotics
- Early mobilization
ERAS: leads to shorter length of stay, reduced nonsurgical complications and no increase in readmission rates.
Resources:
- Full slides (courtesy of Dr. Heiss): ERAS 2016
- Link: ERAS Society website
My take: ERAS concept/team approach is leading to better outcomes. GI surgery is likely to benefit more than other areas due to the often-slow recovery of the GI tract after operations.

Pingback: Top Posts 2016 | gutsandgrowth
Pingback: Ileocecal Resection in Pediatric Crohn’s Disease | gutsandgrowth