
My notes from Georgia Chapter of CCFA’s conference. There could be errors of omission, transcription and/or errors in context based on my understanding.
Evan Feldman, MD –Atlanta Colorectal Surgery
Surgical Management of Fibrostenotic Crohn’s Disease
Key Points:
- Endoscopic dilation (by colorectal surgery or GI) may alleviate symptomatic strictures in selected patients and obviate surgery; dilate to 20 mm if possible. Needs to be a short segment (<5 cm). Consider biopsies to exclude malignancy.
- In adults, higher risk with steroid treatment, particularly if more than 20 mg per day.
- In symptomatic patients who need surgery …Preserve as much small bowel disease as possible. Crohn’s disease is not curable. No need for microscopically-negative disease.
- Stricturoplasty techniques and indications reviewed. No role for stricturoplasty in the colon.
- For gastroduodenal disease, gastrojejunostomy is procedure of choice.
- Discussed perianal fistulas briefly.
- 1st two steps: 1. control sepsis/exam under anesthesia 2. control disease process.
- Then several options: continued use of seton, remove seton and see if better disease control leads to fistula closure, surgical procedure (eg. LIFT procedure) –preferably one with low risk of incontinence. Injection of stem cells (when disease is under control) can be considered but is off-label in U.S. and Dr. Feldman has noted low response rates in his experience.





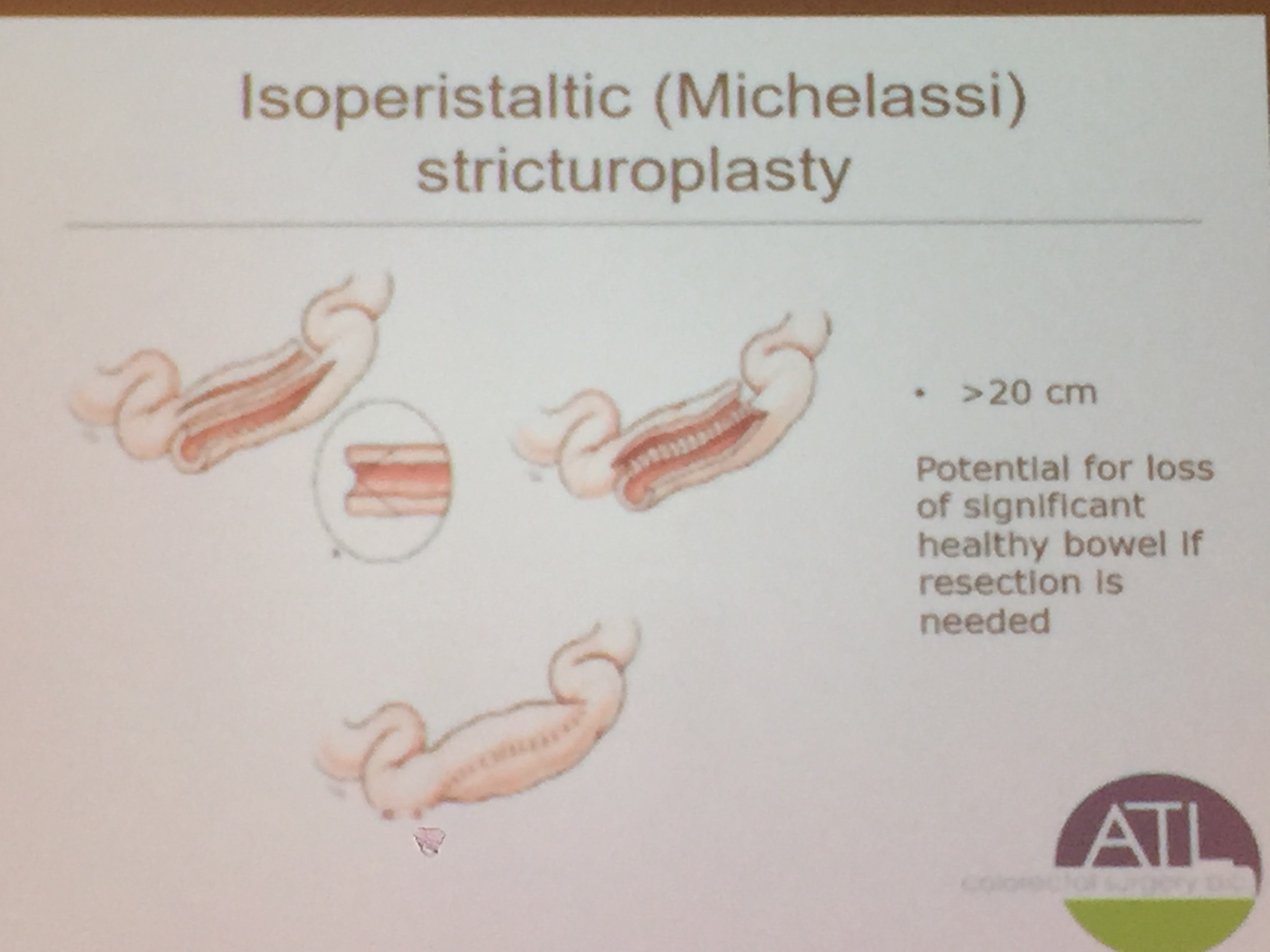
The slide above depicts a Michelassi stricturoplasty which is rarely performed, but considered for long segments of strictured bowel.
Related blog post:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
