
In adults with gastroesophageal reflux, there is more data that magnetic sphincter augmentation (MSA) is a good option for many. R Bell et al. Clin Gastroenterol Hepatol 2020; 18: 1736-1743. Full Text: Magnetic Sphincter Augmentation Superior to Proton Pump Inhibitors for Regurgitation in a 1-Year Randomized Trial)
Methods: Patients with moderate to severe regurgitation (assessed by the foregut symptom questionnaire) despite once-daily PPI therapy (n = 152) were randomly assigned to groups given twice-daily PPIs (n = 102) or laparoscopic MSA (n = 50) at 20 sites.
Key findings:
- MSA resulted in control of regurgitation in 72/75 patients (96%); regurgitation control was independent of preoperative response to PPIs. It is noted that none of the patients in this study had grade C or grade D esophagitis.
- Only 8/43 patients receiving PPIs (19%) reported control of regurgitation.
- In the MSA group, MSA, 61 (81%) had improvements in GERD health-related quality of life improvement scores (greater than 50%) and 68 patients (91%) discontinued daily PPI use. The Demeester scores improved from 33.4 to 3.5 at 6 months post implanation
- Esophageal acid exposure time decreased from 10.7% to 1.3% (P < .001) from study entry to 1-year after MSA.
- Safety: No serious perioperative adverse events occurred in any arm of the study. Although 19 (39.6%) MSA patients and 10 (33.3%) MSA crossover patients reported instances of dysphagia, MSA patients reported less dysphagia at 6 and 12 months than at baseline
Discussion points from authors:
- Relatively limited duration of follow-up, though “other studies of MSA have documented little decrease in efficacy between 1 and 5 years of follow-up”
- The American College of Gastroenterology guidelines indicate “that surgical therapy is not recommended for patients who do not respond to PPI therapy. However, the basis for these recommendations and the types of symptoms evaluated for response to PPI therapy is unclear. Three prospective cohort studies have compared the effectiveness of laparoscopic fundoplication between PPI responsive and nonresponsive populations and found significant symptom improvement with laparoscopic fundoplication in PPI nonresponders, though not quite as much as in PPI responders”
- Increased bloating which is common after laparoscopic fundoplication was not evident with MSA which found a decrease from baseline. “. Continued ability to belch was reported in 99% (n = 74 of 75) of all patients who received MSA at 12 months.”
In the associated editorial, JE Richter (Clin Gastroenterol Hepatol 2020; 18: 1685-1687 Full text: Laparoscopic Magnetic Sphincter Augmentation: Potential Applications and Safety Are Becoming More Clear—But the Story Is Not Over) notes that “erosion and migration of the MSA device have been a rare event thus far. In a total of nearly 10,000 device placements, there were 29 reported cases of erosions…Smaller devices were associated with higher rates of erosions. The 12-bead device was responsible for 18 of 29 erosions (62%) and is no longer available for implantation…To an admitted skeptic about new antireflux treatments, the available data about the symptomatic and
physiological effectiveness, durability, and safety of MSA are very impressive. I believe this procedure now deserves to be routinely done as an alternative surgical procedure to traditional fundoplication for patients with mild-moderate GERD….patients with severe GERD and structural sphincter dysfunction still need the traditional fundoplication”
My take: This study and others shows that MSA (aka Linx) is an effective treatment option for many adult patients with medically-refractory regurgitative reflux.
Related blog posts:
- Stopping reflux with magnets | gutsandgrowth
- Five Year Data on Magnetic Device for GERD
- Transoral Fundoplication for Refractory Gastroesophageal Reflux | gutsandgrowth
- Why didn’t patient with documented reflux get better with …
- How to Make a Study Look Favorable for Reflux Surgery Compared to Medical Treatment
- Surgery for Reflux Works Best in Those Who Need it the Least | gutsandgrowth
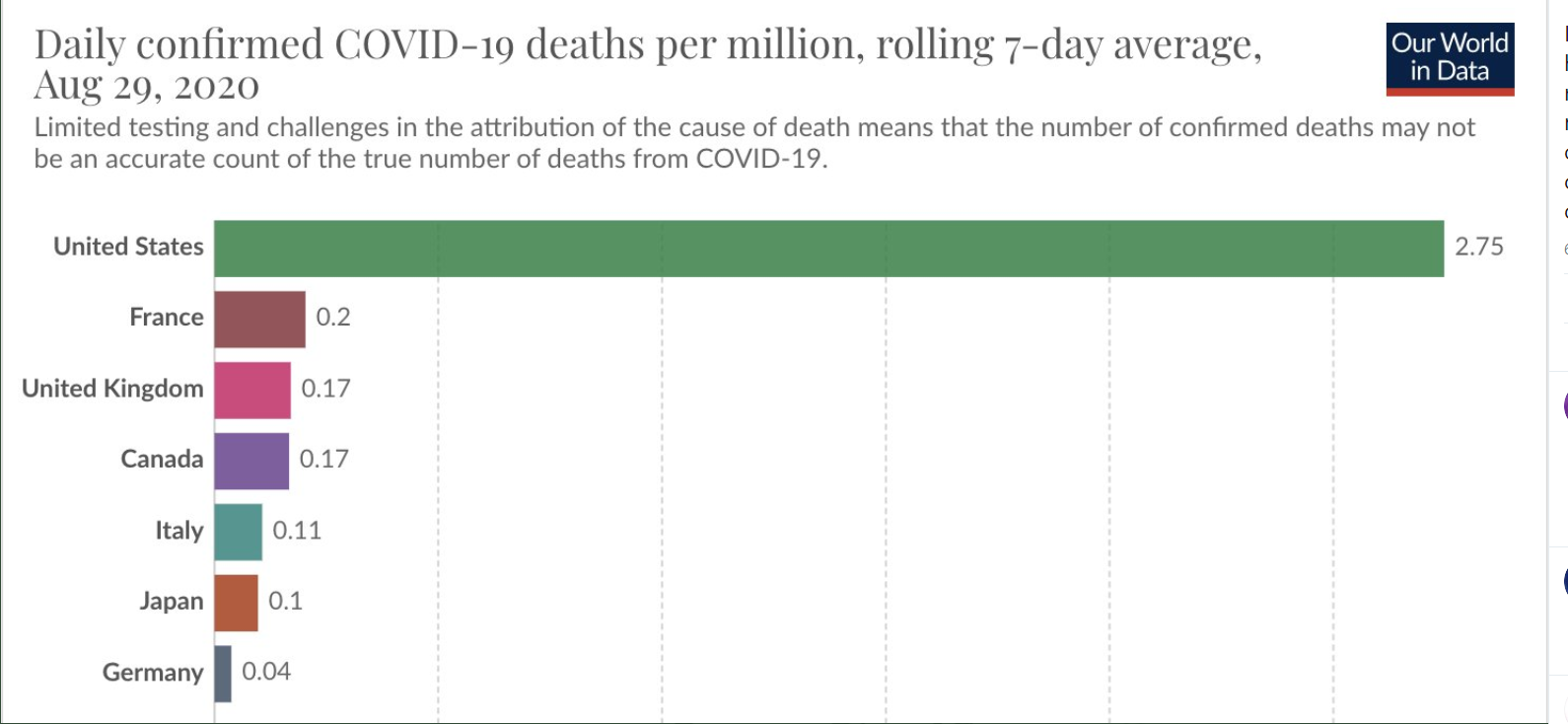

It is surprising to me that almost half of the U.S. thnk that we have handled the pandemic well

