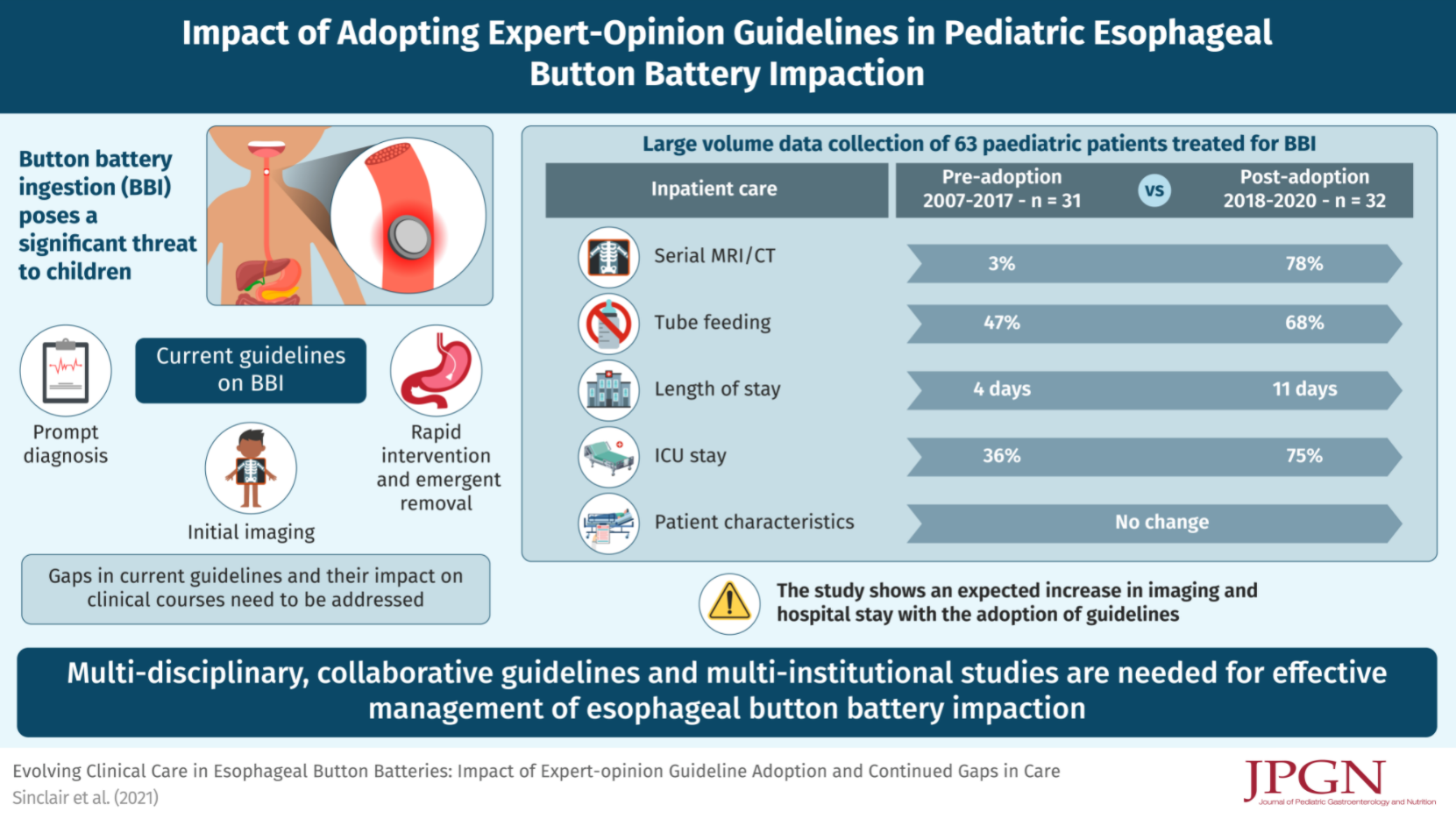
EM Sinclair et al. JPGN 2022; 74: 236-243. This retrospective study (n=63) describes the increased utilization of cross-sectional imaging, adoption of acetic acid irrigations, increased intensive care/hospitalizations after the implementation of consensus institutional guidelines for button battery management (see visual abstract below). An estimate in the increase in costs would have been a good addition to this study.
One of the references (EM Sinclair et al. J Pediatr Surg Case Rep 2021; 66: 101782. doi: 10.1016/j.epsc.2021.101782. Open Access: Development and repair of aorto-esophageal fistula following esophageal button battery impaction: A case report) describes one of the goals of prolonged hospitalization, namely preventing catastrophic bleeding. In this case report, though, the 6 yo had been discharged 12 days after presentation and represented on day 25 with hematemesis from a new aorto-esophageal fistula, requiring emergent cardiac catheterization with successful, life-saving aortic stent placement; “however a multidisciplinary approach to procedure planning is necessary with availability of surgical support for open repair if necessary.” This report has a lot of good images. The discussion notes that the National Capital Poison Center (NCPC) database reports a total 64 deaths in children following button battery ingestion worldwide since 1977; 61% (39/64) of which were due to documented arterio-esophageal fistulae (the actual numbers of deaths is likely much higher). This report also highlights the fact that serial MRIs “may not predict the development of severe complications.”
Related blog posts:
- Foreign Bodies in Children -Expert Guidance Even with “spent” batteries, there is enough residual charge to cause injury and all ingestions (even if asymptomatic) into the esophagus require emergent removal. If these batteries are in the stomach & asymptomatic, urgent removal is recommended if age < 5 years and BB ≥20 mm.
- New Button Battery Guidelines -with honey and vinegar
- Button battery -Update For Families
- Do Button Battery Guidelines Need to be Updated?