
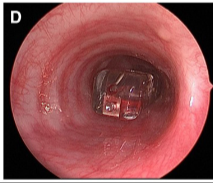
A Andreoli et al. JPGN Report 2023; DOI: 10.1097/PG9.0000000000000299 Open Access! Foreign Body in the Bronchus Intermedius: Inadvertent Deployment of a Bravo Wireless pH Probe in the Airway
This case report describes placement of a Bravo pH capsule into the bronchus rather than in the esophagus. The complication was quickly recognized and managed by having ENT remove the capsule during the same anesthetic. It is noted that the esophageal mucosal findings included “longitudinal furrows, edema, and mucosal friability.” Biopsies “demonstrated esophagitis consistent with GER.”
Key point:
- The authors note that this has led to a change in their practice: “before suction attachment, the endoscope is reintroduced into the hypopharynx to ensure the delivery system enters the cricopharyngeus. This ensures esophageal probe placement before deployment.”
My take: It has been my practice since the Bravo catheter’s inception to assure the deployment catheter is in the esophagus before releasing the Bravo capsule. However, I am impressed with this report. It is very helpful for practitioners to relay difficult experiences to help others avoid complications. This case report should be a reminder also to carefully consider whether a pH study is needed in those with erosive esophagitis.
Related blog posts:
- Good Episode of Bowel Sounds on Reflux
- AGA Expert Clinical Practice Update for Adults with GERD (2022)
- pH Probe Testing: Rumors of My Death are Premature
- Why Vonoprazan Is More Effective For Erosive Esophagitis Than a Proton Pump Inhibitor
- Which Proton Pump Inhibitor is the Most Potent?
Related article: Open Access! Hochman JA, Favaloro-Sabatier J. Tolerance and reliability of wireless pH monitoring in children. J Pediatr Gastroenterol Nutr 2005; 41:411–415.
