This blog entry has abbreviated/summarized these presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
This is a long post –highlighting four separate talks on eosinophilic esophagitis.
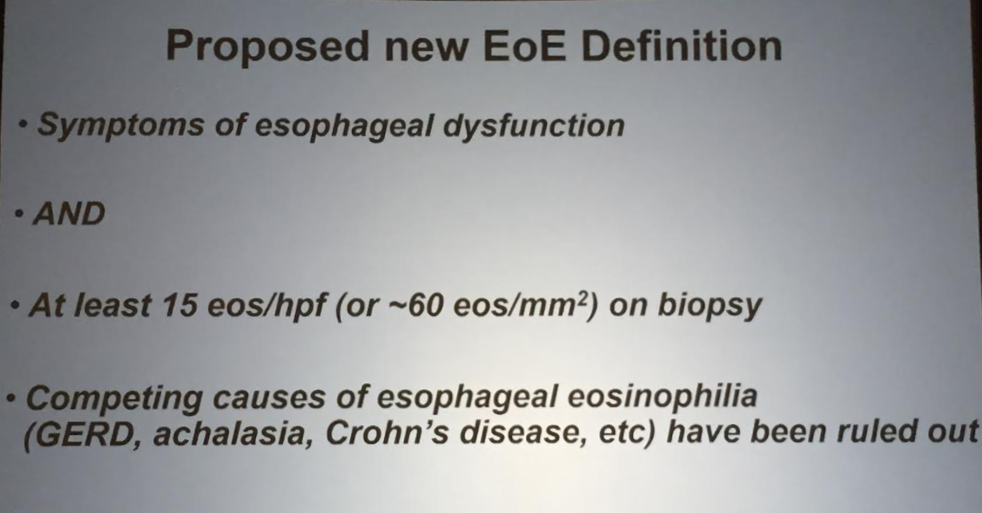
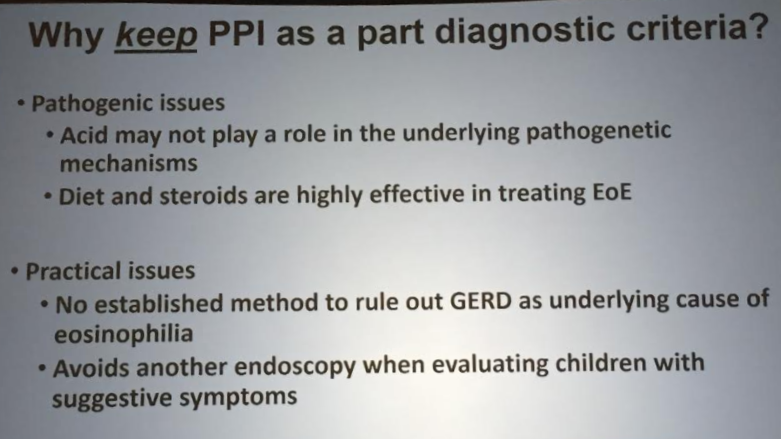
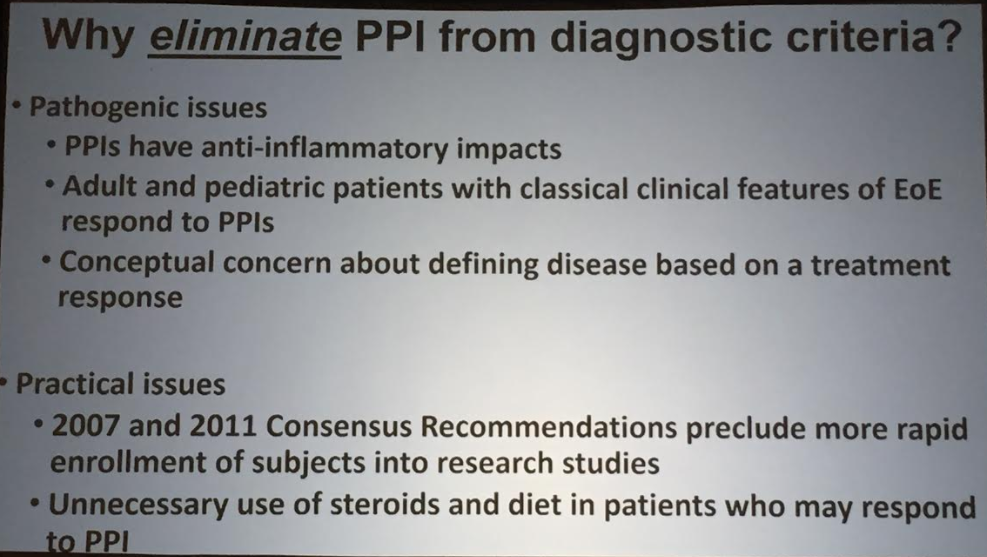
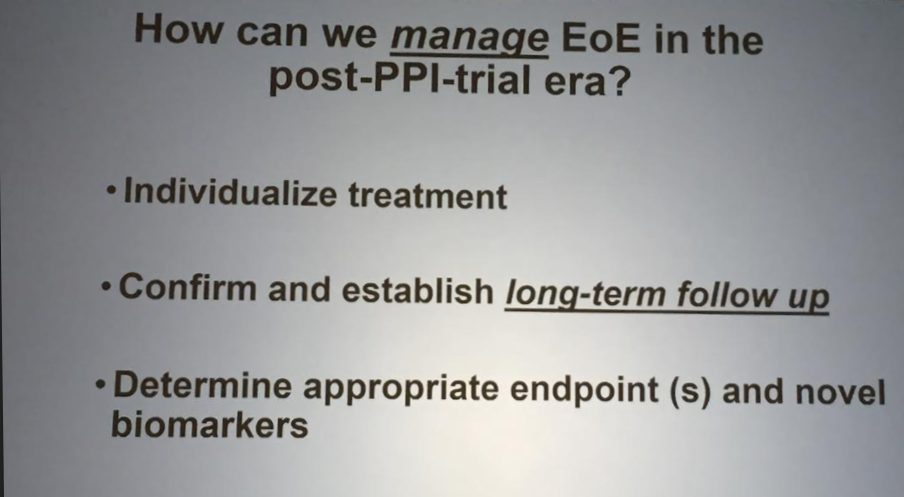
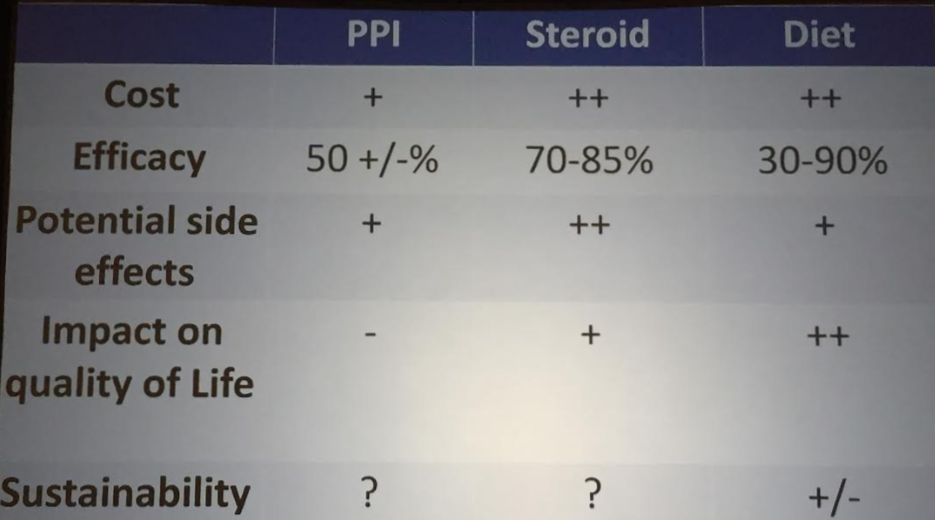
PPI Use in Esophageal Eosinophilia: Recommendations from the recent AGREE conference
Glenn Furuta Children’s Hospital of Colorado
Key points:
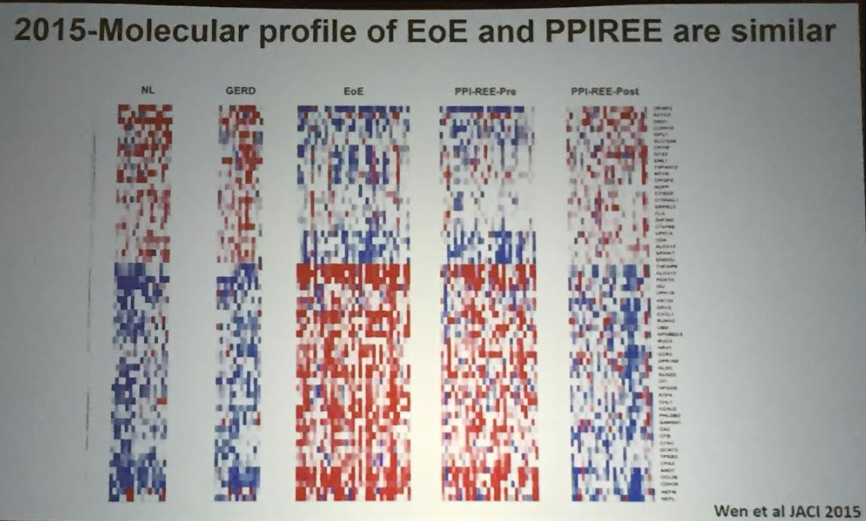
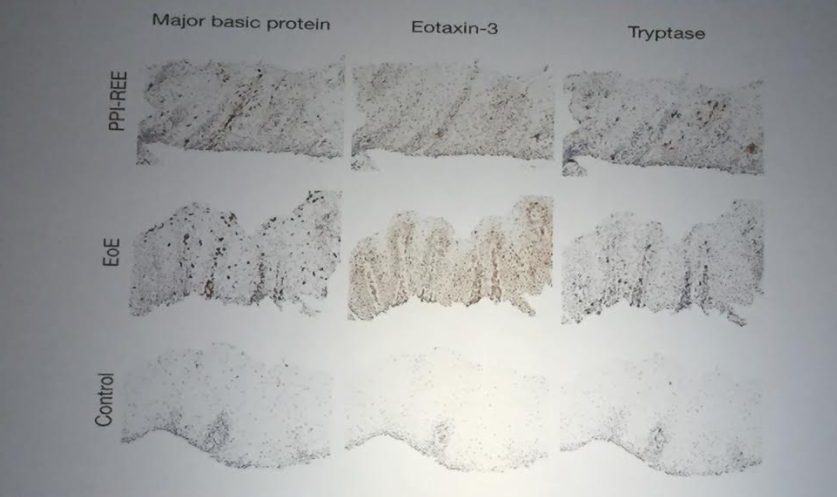
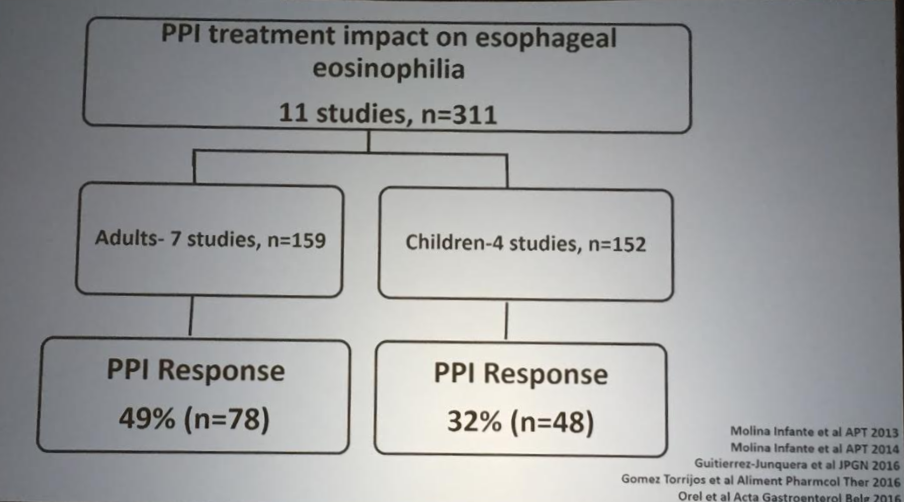
The term PPI-REE (proton pump inhibitor-responsive eosinophilic esophagitis) may not be needed. PPI-REE is quite similar to eosinophilic esophagitis based on molecular and clinical features. The main difference being that this subset responds to PPI therapy.


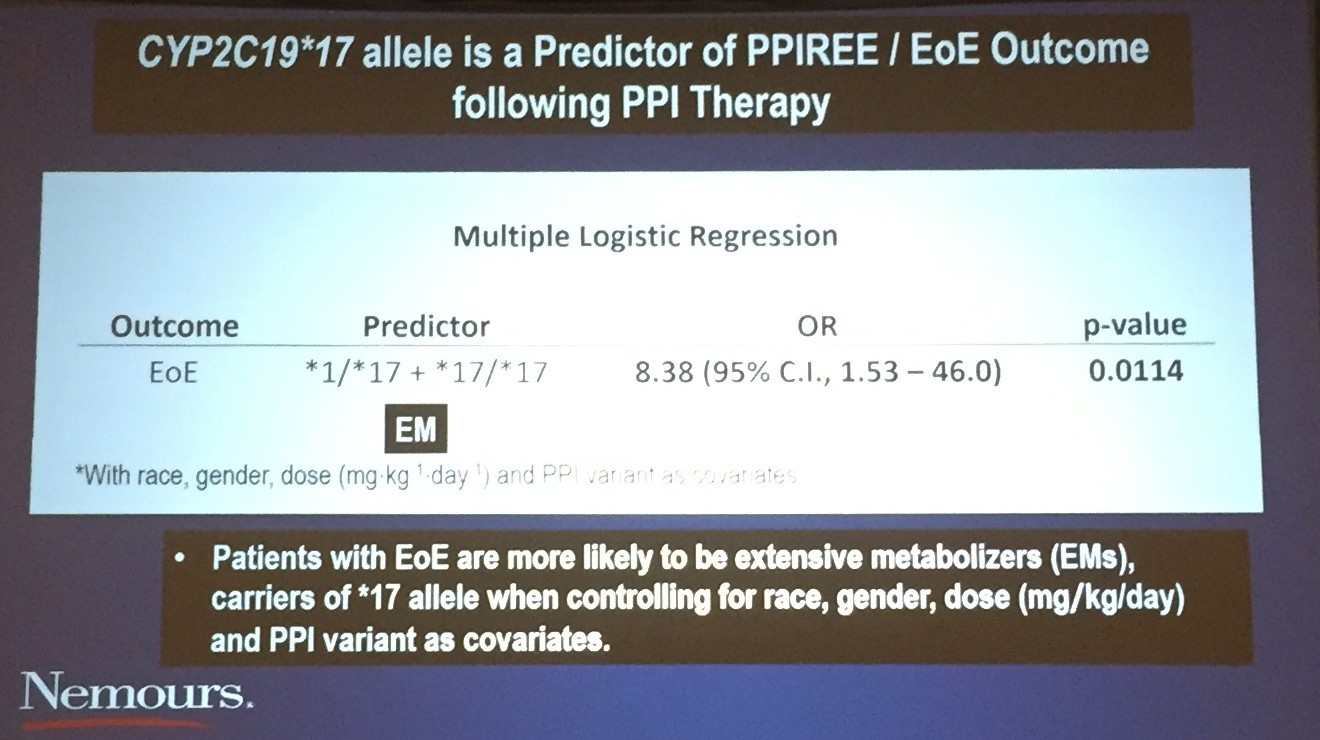
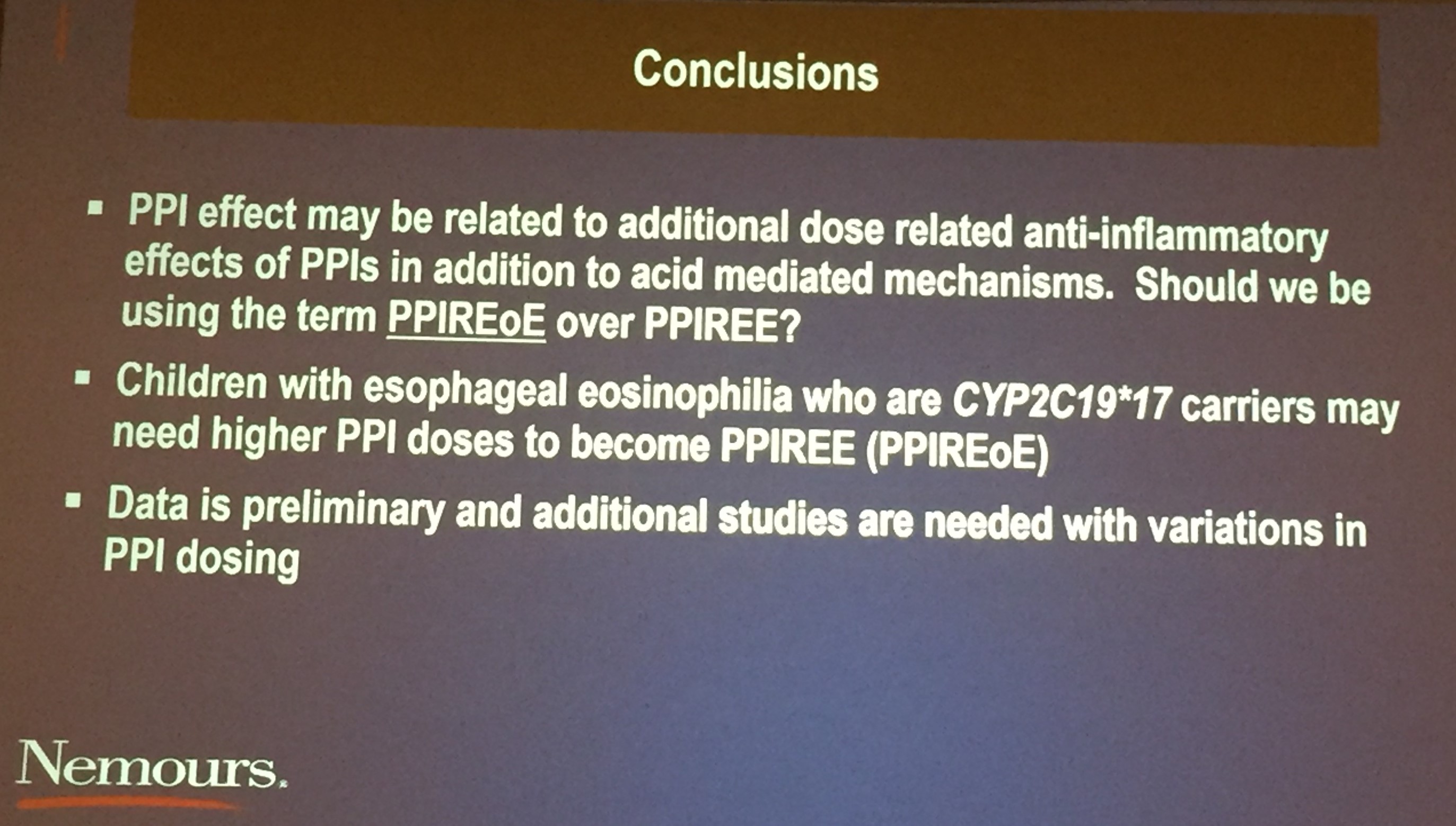
Characterization of CYP2C19*17 Polymporphisms Among Children with PPI Responsive EoE and EoE
James Franciosis et al. Nemours Children’s Hospital Orlando
My take: This cool presentation offered a potential explanation of why some patients respond to PPIs (so called “PPI-REE”) from those with EoE that does not respond to PPIs. This is pertinent because on a molecular basis the disease appears to be the same. The difference in PPI-REE from EoE may be how the patient metabolizes PPI. Those EoE patients who metabolize PPIs “extensively” are much less likely to respond to this therapy.

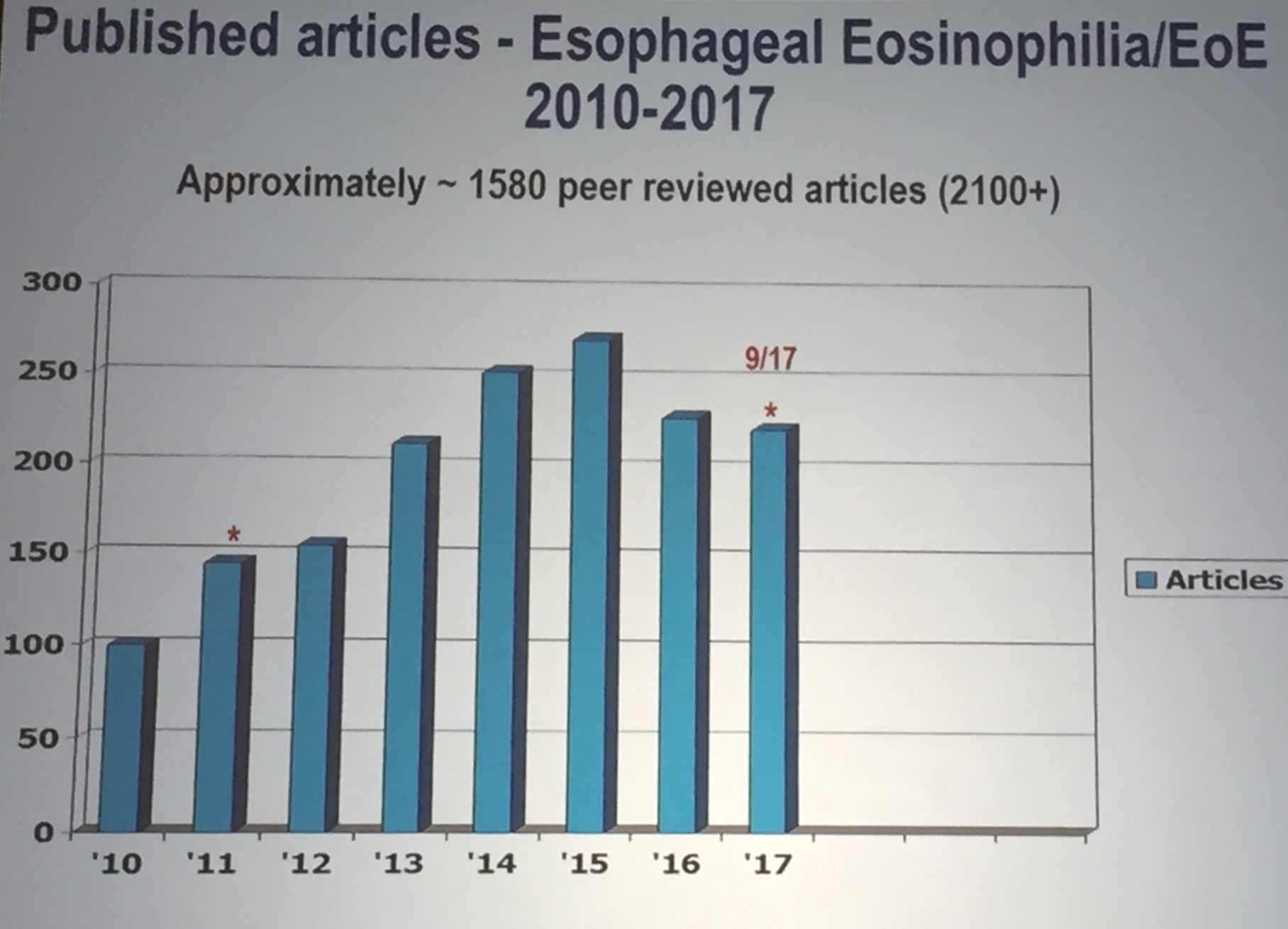
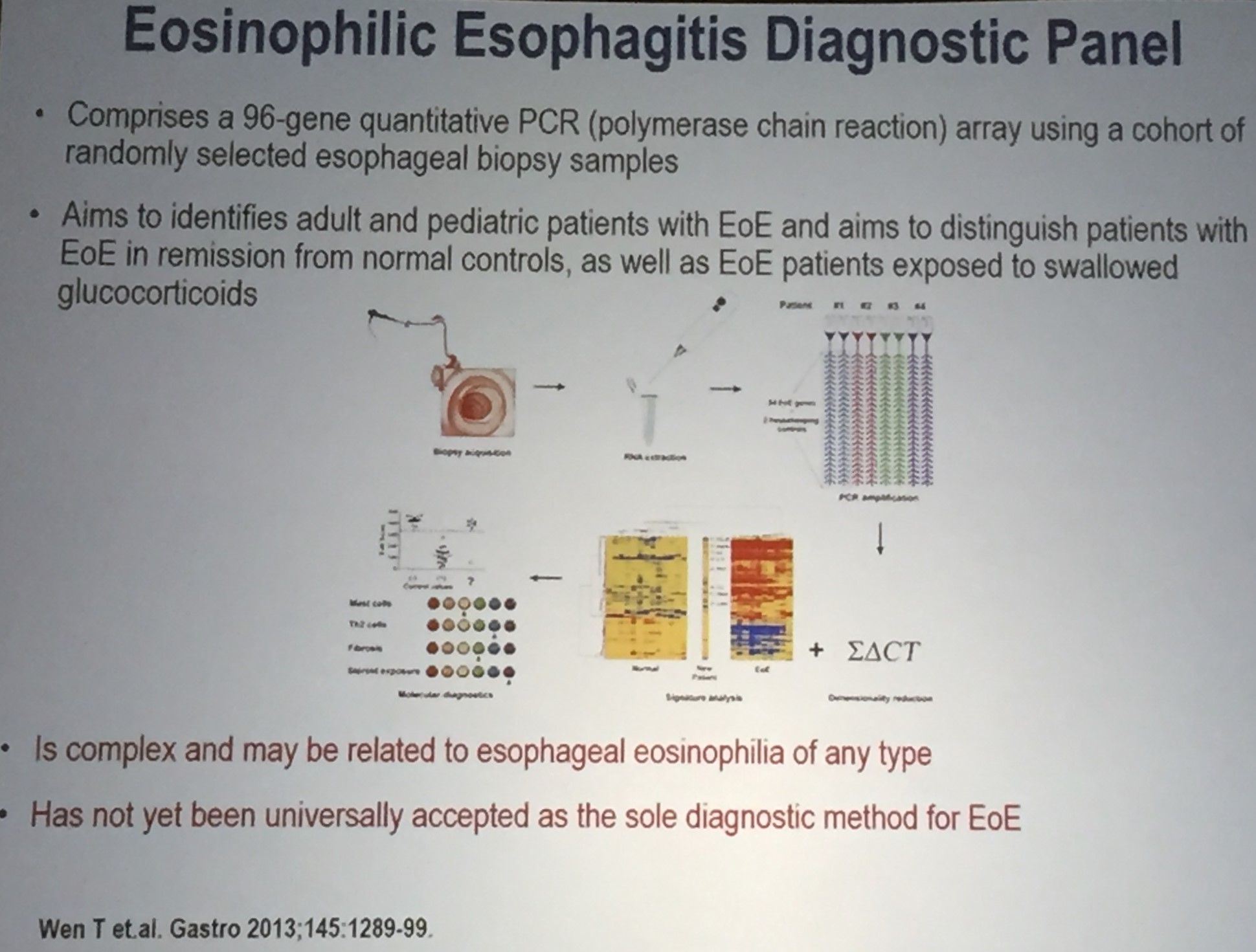
Eosinophilic esophagitis: Now an “Oldie” -But with increased interest and new research, a “Goodie”
Chris Liacouras Children’s Hospital of Philadelphia
This lecture covered an enormous amount of material. Here are a few slides.

Final Lecture (from November 3rd presentation):
Key points:
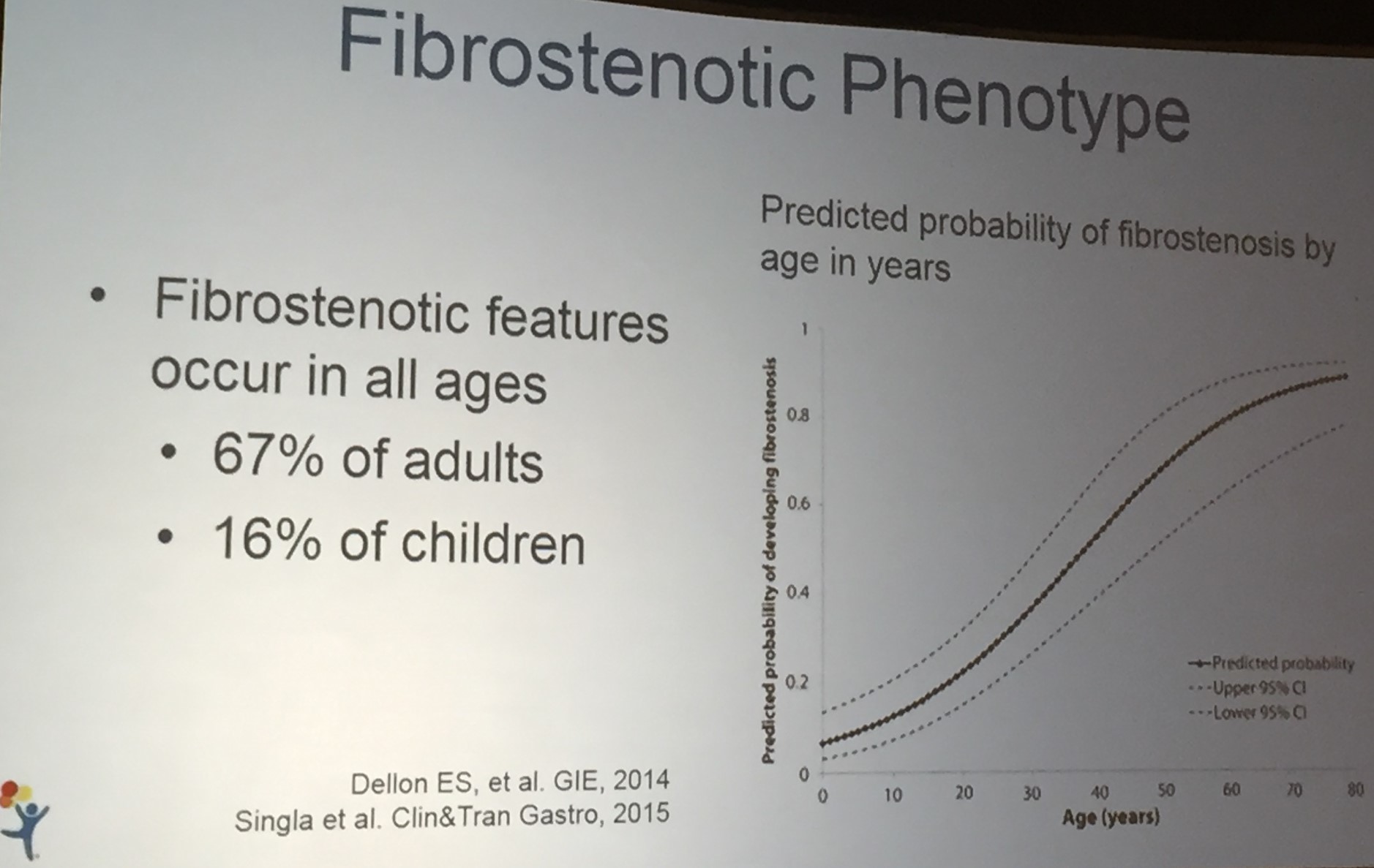
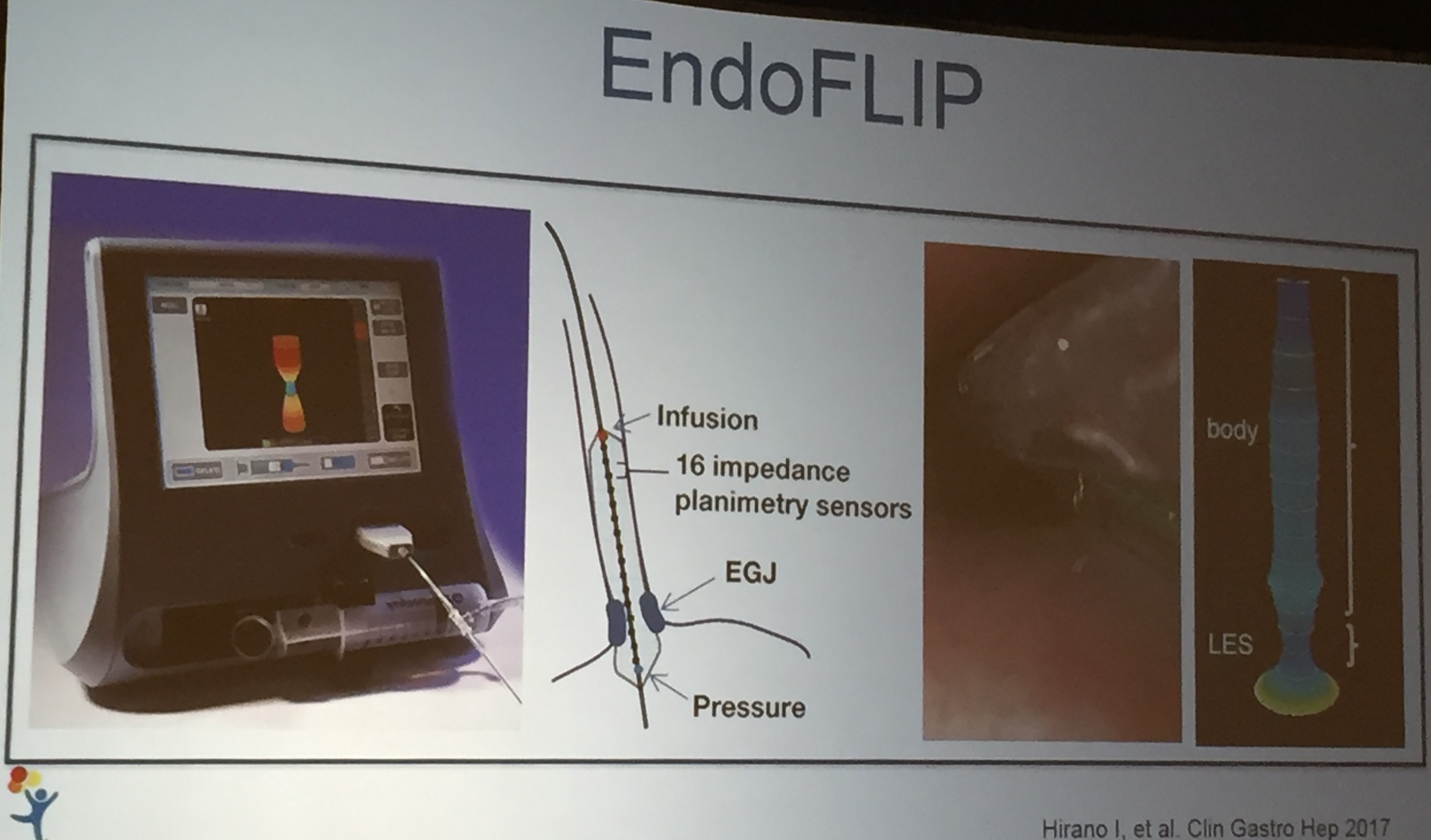
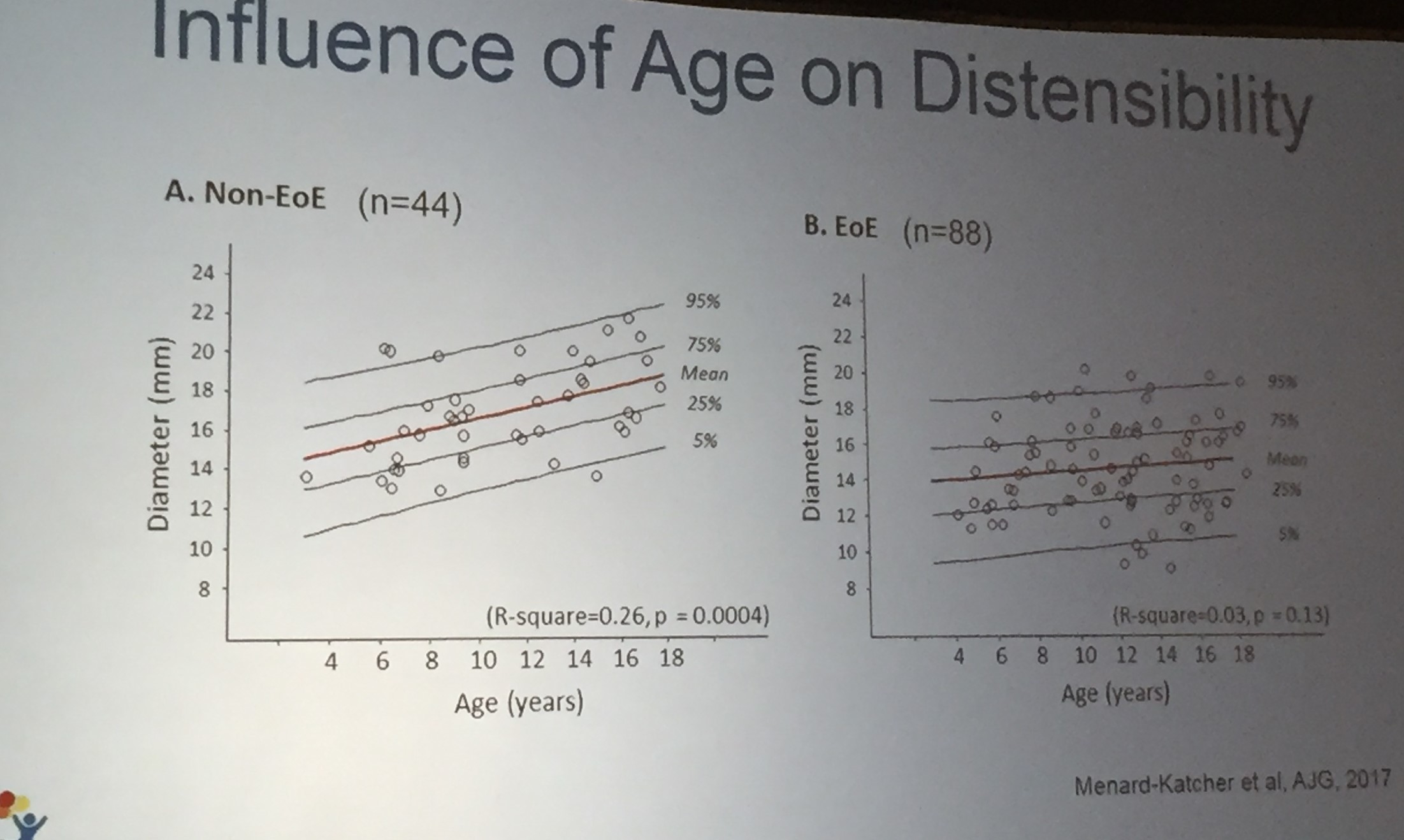
- Endoflip is a new tool that helps determine esophageal distensibility. Improved distensibility indicates less fibrostenotic disease which is one long-term goal.
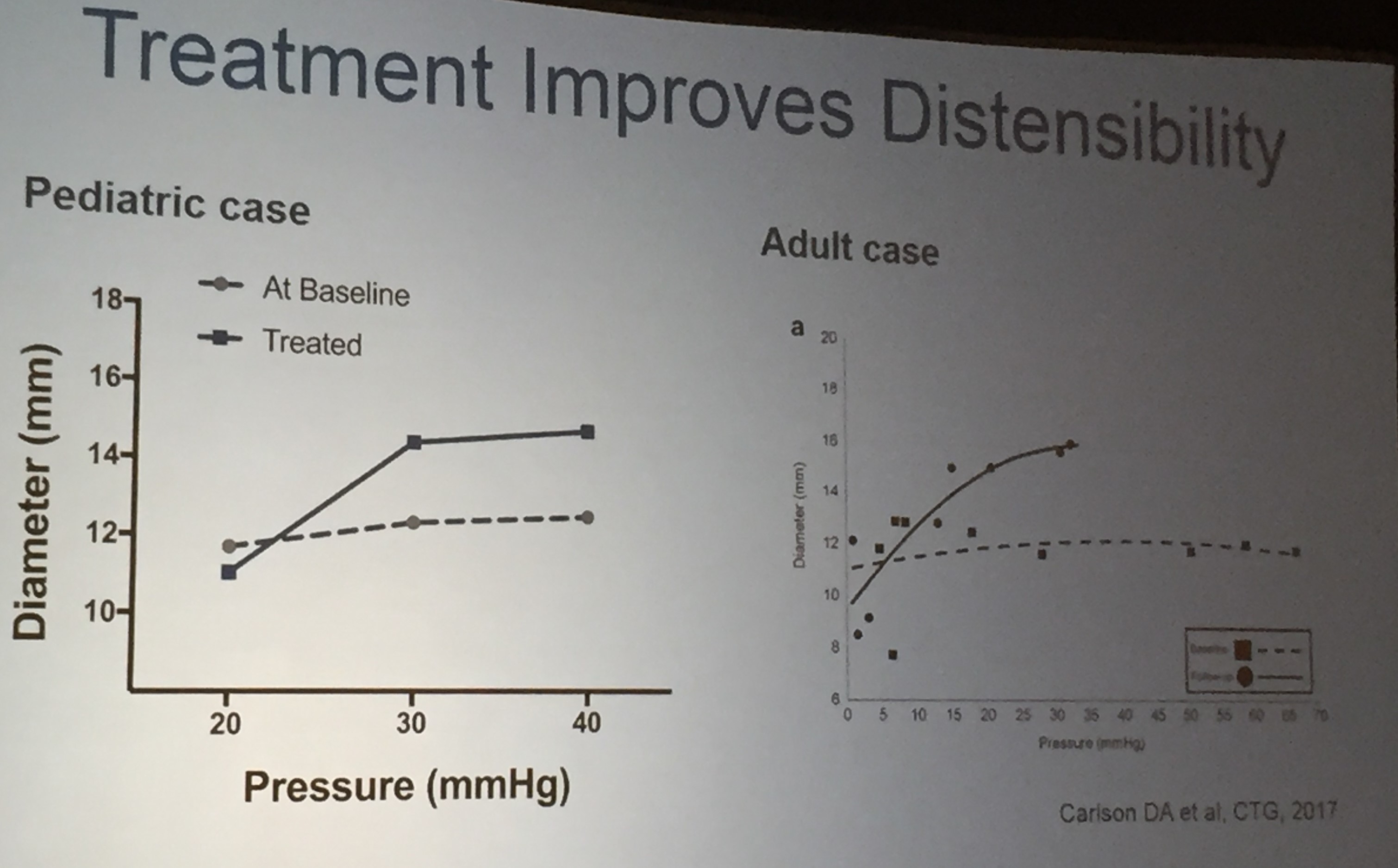
- Response to treatment has been correlated in improvement in Endoflip measurements.
- There are no FDA approved medications at this point for EoE, though topical steroids may be approved soon.