
A recent study for optimizing infliximab dosing: LE Bauman et al. Inflamm Bowel Dis. 2019 Jul 9. pii: izz143. doi: 10.1093/ibd/izz143. [Epub ahead of print]
The authors identified 228 pediatric patients with IBD and developed a pharmocokinetic model using weight, albumin, sedimentation rate and antibodies to infliximab (ATI) to help predict infliximab dosing that would achieve a therapeutic trough level (>5 mcg/mL).
In their study, they also simulated 1000 patients and found that only 24% of patients receiving 5 mg/kg q8weeks achieved a therapeutic level; this increased to 56% for 10 mg/kg q8weeks. Shortening dose interval more reliably achieved therapeutic levels: 5 mg/kg q4 weeks had a target level in 84% and 10 mg/kg q6 weeks had a target level in 80%.
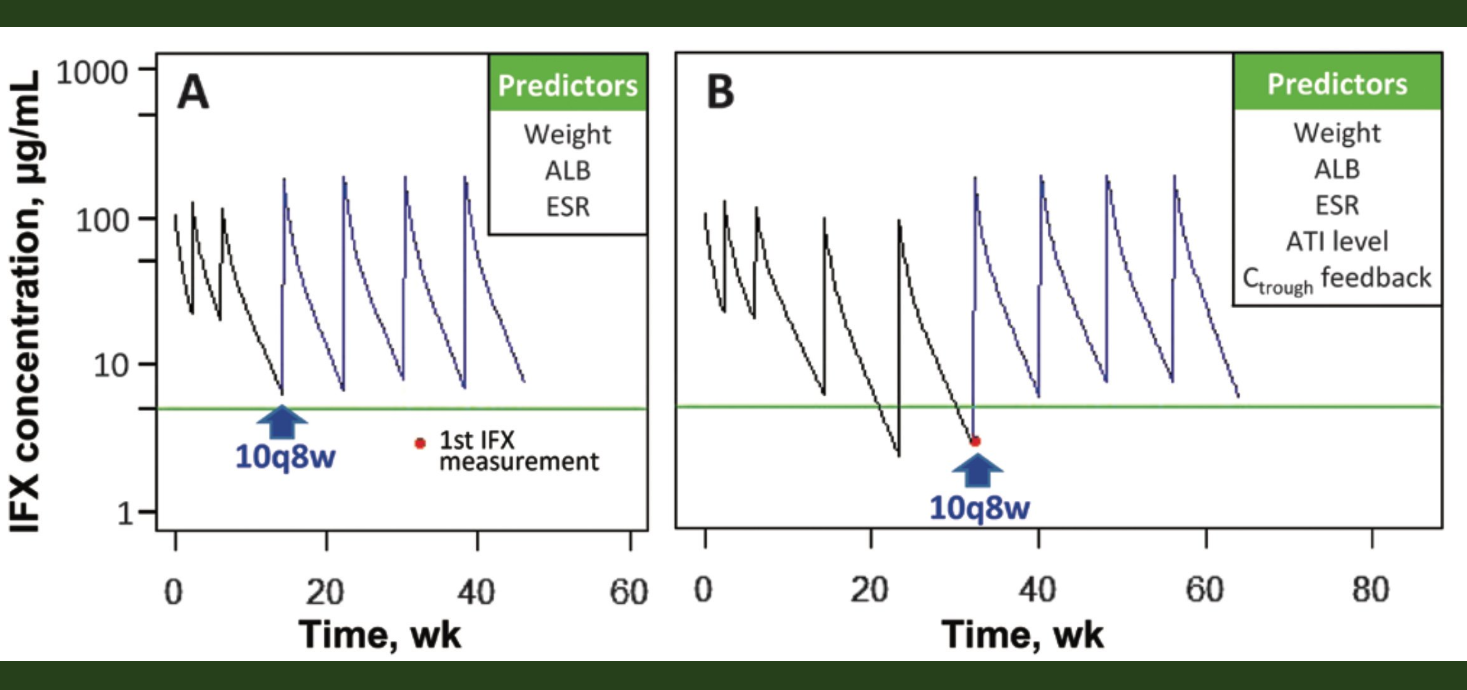
The image above corresponds to Figure 5 in the manuscript. This figure shows the difference between proactive and reactive dosing strategy. In the first panel, a higher initial dose prevents suboptimal dosing whereas the second panel shows suboptimal troughs until adjustment of dose after identifying a low trough. Avoiding low troughs may reduce the likelihood of developing antibodies to infliximab and therapeutic failure
My take: This study and several others indicate that most pediatric patients need either more frequent inflixmab dosing or higher initial doses to achieve therapeutic levels and to improve outcomes.

Pingback: How Much Infliximab Can You Give to Young Children? | gutsandgrowth